As of May 2026, millions of Americans relying on Medicaid face a shifting landscape of cost-sharing requirements—thanks to sweeping changes enacted under the 2025 Inflation Reduction Act (IRA) reconciliation provisions. While Medicaid traditionally provided free or low-cost coverage to eligible individuals, recent policy updates have introduced premiums, deductibles, and copays for certain beneficiaries, particularly those earning above specific income thresholds. For health journalists and policymakers tracking these developments, the implications are far-reaching: from patient access to healthcare services to state budget allocations and federal compliance.
Dr. Helena Fischer, Editor of Health at World Today Journal, breaks down the key changes, their impact on beneficiaries, and what stakeholders should watch for in the coming months. With Medicaid covering over 90 million Americans—including low-income adults, children, pregnant women, and individuals with disabilities—understanding these policy shifts is critical for both providers and patients navigating the system.
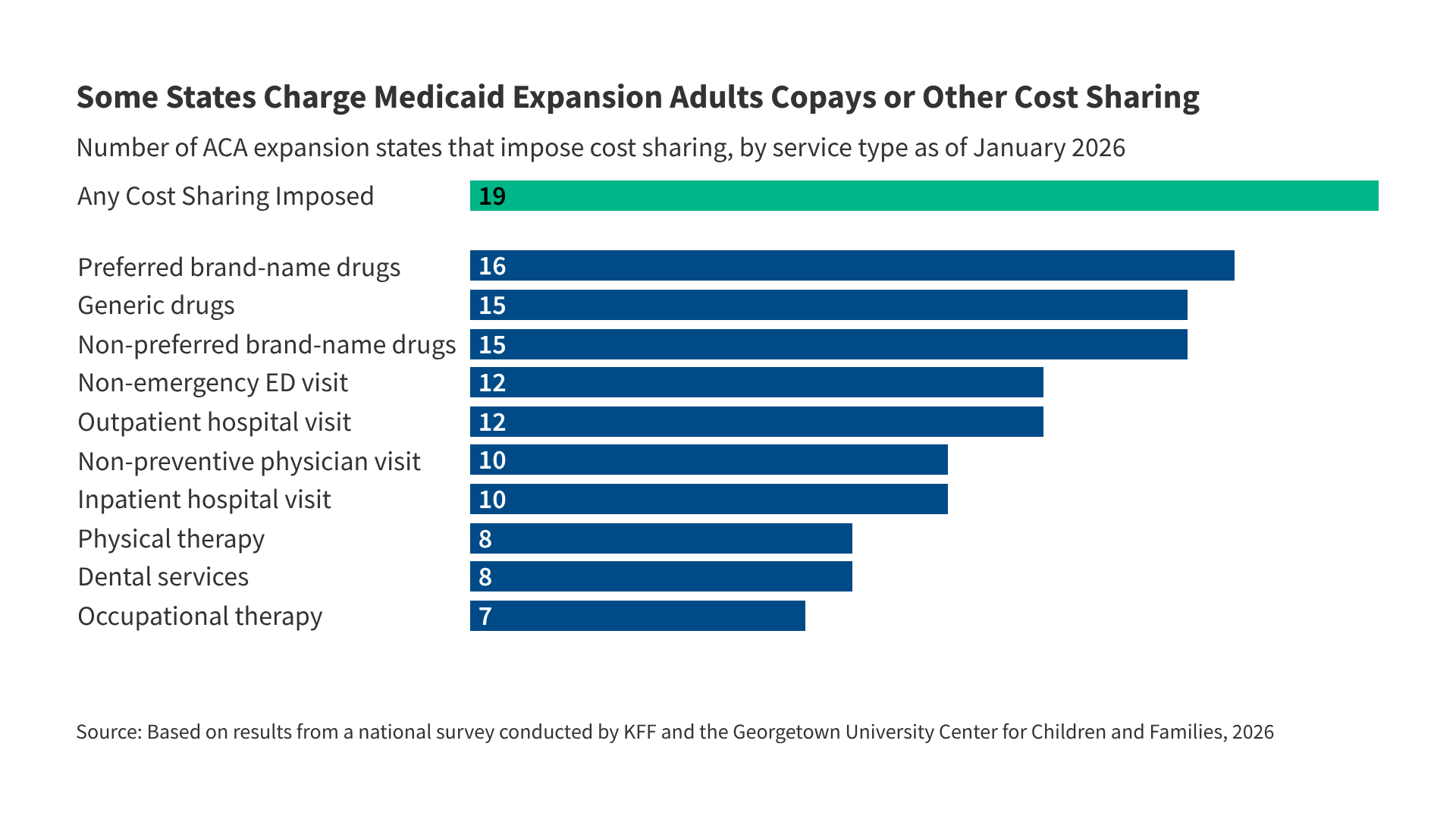
The 2025 reconciliation law marked the first major federal expansion of Medicaid cost-sharing in over a decade. While the Affordable Care Act (ACA) had previously limited cost-sharing for certain groups, the new provisions now allow states to impose premiums, deductibles, and copayments on non-disabled adults earning above 133% of the federal poverty level (FPL). This shift reflects broader fiscal pressures on state budgets and ongoing debates about balancing affordability with sustainability in public health programs.
What Are Medicaid Cost-Sharing Rules?
Medicaid cost-sharing refers to the out-of-pocket expenses beneficiaries may incur when accessing healthcare services. Traditionally, Medicaid has covered nearly all costs for eligible individuals, but recent changes have introduced new financial responsibilities. Key components now include:
- Premiums: Monthly fees paid by beneficiaries to maintain coverage.
- Deductibles: Annual amounts beneficiaries must pay before insurance coverage begins.
- Copayments: Fixed fees for specific services, such as doctor visits or prescriptions.
Before 2025, federal law prohibited Medicaid from imposing premiums, deductibles, or copayments on most beneficiaries. However, the 2025 Inflation Reduction Act amended Section 1902 of the Social Security Act to permit these cost-sharing mechanisms for non-disabled adults earning above 133% of the FPL. States now have the flexibility to design their own cost-sharing structures, provided they comply with federal guidelines on affordability and equity.
For example, a beneficiary earning $20,000 annually (133% of the 2025 FPL for a single individual) may now face premiums of up to $15 per month, depending on their state’s policies. While this amount may seem modest, the cumulative impact on low-income households—where every dollar counts—can be significant. Deductibles of up to $1,000 per year and copayments capped at 5% of the service cost (with some exceptions for essential health benefits) further shape the financial burden.
Key Changes from the 2025 Reconciliation Law
The 2025 reconciliation law introduced three primary modifications to Medicaid cost-sharing rules:

- Expanded Eligibility for Cost-Sharing: States can now impose cost-sharing on non-disabled adults with incomes above 133% of the FPL, a threshold previously reserved for Marketplace plans under the ACA.
- State Flexibility: States determine the types and amounts of cost-sharing, subject to federal limits. For instance, some states may opt for premiums only, while others combine premiums with deductibles and copayments.
- Protective Safeguards: Cost-sharing cannot exceed 5% of monthly income for beneficiaries earning up to 200% of the FPL, and states must ensure that cost-sharing does not exceed 10% of income for those earning between 200% and 250% of the FPL.
These changes reflect a deliberate shift toward shared responsibility in Medicaid financing, aligning the program more closely with private insurance models. However, critics argue that the new rules risk disproportionately burdening low-income individuals who may struggle to afford additional out-of-pocket expenses. Supporters, meanwhile, contend that cost-sharing incentivizes beneficiaries to use healthcare services more judiciously and reduces long-term strain on state budgets.
State-Level Variations: How Policies Differ Across the U.S.
As of May 2026, states have adopted varying approaches to Medicaid cost-sharing under the new federal guidelines. While some states have implemented modest premiums or copayments, others have chosen to maintain traditional fee-for-service models with minimal cost-sharing. Below is a snapshot of how selected states are applying the new rules:
| State | Cost-Sharing Type | Income Threshold for Cost-Sharing | Maximum Monthly Premium | Deductible Cap (Annual) | Copayment Cap |
|---|---|---|---|---|---|
| California | Premiums + Copayments | 133%–200% FPL | $10–$25 | $500 | 5% of service cost |
| Texas | Premiums Only | 150%+ FPL | $5–$15 | None | None |
| New York | Premiums + Deductibles | 133%–250% FPL | $12–$30 | $750 | 5% of service cost |
| Florida | No Cost-Sharing | N/A | None | None | None |
| Ohio | Premiums + Copayments | 133%–200% FPL | $8–$20 | $600 | 5% of service cost |
Note: States like Florida have opted out of imposing cost-sharing entirely, while others, such as California and New York, have adopted more comprehensive models. The Centers for Medicare & Medicaid Services (CMS) continues to monitor state implementations to ensure compliance with federal affordability standards.
For beneficiaries, these variations mean that financial responsibility for healthcare can differ dramatically depending on where you live. For example, a resident of California earning $22,000 annually (150% FPL) might pay up to $25 per month in premiums plus copayments for services, whereas a similarly situated resident in Texas could pay as little as $5 per month. This disparity underscores the importance of understanding state-specific policies when navigating Medicaid enrollment.
Who Is Affected by These Changes?
The 2025 Medicaid cost-sharing reforms primarily impact the following groups:
- Non-Disabled Adults: Individuals without disabilities earning above 133% of the FPL are now subject to cost-sharing requirements in states that have implemented them.
- Low-Income Workers: Many beneficiaries in this category work part-time or in low-wage jobs, making additional out-of-pocket costs particularly challenging.
- Parents and Caregivers: Families relying on Medicaid for children’s healthcare may face new financial burdens if they fall into the cost-sharing income brackets.
- States and Providers: Healthcare providers must adjust billing practices to accommodate new cost-sharing structures, while states grapple with balancing revenue needs and beneficiary access.
One group largely exempt from cost-sharing under the new rules includes:
- Children
- Pregnant women
- Individuals with disabilities
- Beneficiaries earning below 133% of the FPL
These exemptions reflect federal priorities to protect vulnerable populations from additional financial barriers to care. However, advocates warn that even modest cost-sharing requirements could deter some individuals from seeking preventive or routine care, potentially worsening long-term health outcomes.
What Does the Research Say About Cost-Sharing?
Studies on Medicaid cost-sharing offer mixed insights into its impact on healthcare utilization and financial well-being. Key findings include:
- Reduced Service Use: Research published in Health Affairs (2024) found that Medicaid beneficiaries subject to cost-sharing were 10–15% less likely to seek non-emergency care, including preventive services like annual check-ups and screenings. This trend is particularly concerning for chronic disease management, where early intervention can prevent costly complications.
- Financial Strain: A 2025 report from the Urban Institute estimated that households earning between 133% and 200% of the FPL could face additional healthcare expenses of $300–$600 annually due to cost-sharing. For families living paycheck to paycheck, this represents a meaningful share of their income.
- State Budget Relief: Proponents argue that cost-sharing generates additional revenue for states. For example, California projected $120 million in annual savings from premiums alone, though these savings must be weighed against potential reductions in service utilization.
Dr. Fischer notes that the long-term effects of cost-sharing remain uncertain, particularly as states continue to refine their policies. “What we do know is that Medicaid plays a critical role in safety-net healthcare,” she says. “Any policy that increases financial barriers risks creating new disparities in access—especially for populations already struggling to afford basic needs.”
Practical Steps for Beneficiaries
If you or someone you know is affected by the new Medicaid cost-sharing rules, here’s what to do:
- Check Your State’s Policies: Visit your state Medicaid agency’s website (e.g., Medicaid.gov) to confirm whether cost-sharing applies to your income level.
- Review Your Bill: Pay close attention to premium notices and deductible requirements. Some states provide hardship exemptions for beneficiaries who cannot afford cost-sharing.
- Explore Assistance Programs: Many states offer sliding-scale fee assistance or charity care programs to help offset costs. Ask your healthcare provider or local social services office for details.
- Appeal Denials: If you believe cost-sharing is causing undue hardship, you may be eligible to appeal the decision through your state’s Medicaid office.
- Stay Informed: Cost-sharing rules may evolve as states adjust their programs. Bookmark resources like the CMS Medicaid Cost-Sharing Guide for updates.
For those concerned about affordability, it’s also worth exploring whether Marketplace plans under the ACA might offer more predictable costs, depending on your income and location.
Key Takeaways
- The 2025 Inflation Reduction Act allows states to impose cost-sharing on Medicaid beneficiaries earning above 133% of the FPL for the first time.
- Cost-sharing includes premiums, deductibles, and copayments, with federal limits to protect low-income households.
- States have wide discretion in designing cost-sharing structures, leading to significant variations across the U.S.
- Research suggests cost-sharing may reduce healthcare utilization, particularly for preventive services, while generating revenue for states.
- Beneficiaries should verify their state’s policies, explore assistance programs, and monitor bills for cost-sharing notices.
What’s Next? Monitoring the Impact
As states finalize their cost-sharing implementations, several developments will shape the future of Medicaid:

- CMS Oversight: The Centers for Medicare & Medicaid Services will continue to review state plans to ensure compliance with federal affordability standards. Any violations could trigger corrective actions or funding reductions.
- Beneficiary Feedback: States may adjust their cost-sharing policies based on enrollment data and beneficiary complaints. For example, if premiums lead to high disenrollment rates, states might lower fees or expand exemptions.
- Legislative Reforms: Advocacy groups, including the National Health Law Program and Center on Budget and Policy Priorities, are pushing for additional safeguards to protect vulnerable populations. Watch for potential federal or state legislation in 2027.
- Data Collection: CMS and state agencies will track long-term impacts on healthcare access, financial burden, and overall health outcomes. Early data releases are expected in late 2026 or early 2027.
The next major checkpoint will be the release of CMS’s 2027 Medicaid Cost-Sharing Compliance Report, scheduled for September 2027. This report will provide a national snapshot of how states have implemented the new rules and whether they have achieved their intended fiscal and utilization goals.
Have Questions or Experiences to Share?
Medicaid cost-sharing is a complex and evolving topic. If you’re a beneficiary navigating these changes, a healthcare provider adjusting to new billing practices, or a policymaker tracking state implementations, we’d love to hear from you. Share your insights in the comments below or email [email protected].
For official updates, bookmark the CMS Medicaid website and your state’s Medicaid agency. Stay informed, stay engaged, and let’s continue the conversation about how to make healthcare more accessible for all.
Keep reading