Immigrants play a critical role in stabilizing the United States healthcare system, particularly within the nursing and long-term care sectors. Foreign-born professionals comprise a significant portion of the nation’s doctors, nurses, and support staff, helping to mitigate chronic labor shortages and meet the rising medical demands of an aging population.
The U.S. healthcare system currently faces a dual challenge: an aging domestic population requiring more intensive medical attention and a shrinking supply of domestic healthcare workers. Data from the Bureau of Labor Statistics and various healthcare advocacy groups suggest that immigrant labor is no longer just a supplement to the workforce but a foundational component of its stability. Without foreign-born clinicians and caregivers, many hospitals and long-term care facilities would likely face immediate operational crises.
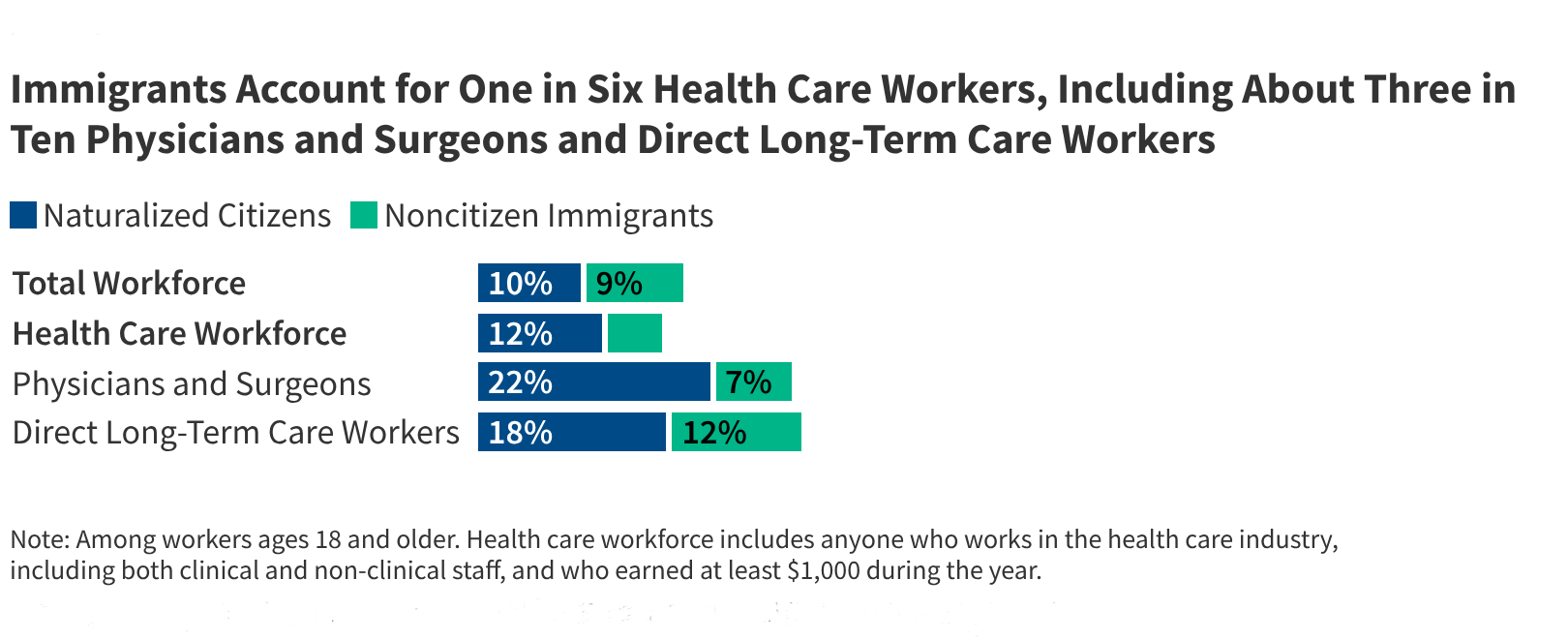
This reliance spans the entire spectrum of care, from highly specialized surgeons and diagnostic physicians to the direct care workers who provide essential daily assistance in nursing homes. As healthcare policy debates continue in Washington, the intersection of immigration law and medical staffing has become a central concern for hospital administrators and public health officials alike.
How many immigrants currently work in the U.S. healthcare sector?
While exact, real-time numbers fluctuate due to varying census methods and visa statuses, immigrants represent a substantial percentage of the total healthcare workforce. According to data analyzed by the American Medical Association and various demographic studies, foreign-born physicians and nurses are distributed across every state, though they are often concentrated in urban medical hubs or specific regions facing acute shortages.
Medical professionals who are international medical graduates (IMGs) are particularly vital. The Association of American Medical Colleges (AAMC) has frequently noted that IMGs are essential for filling gaps in primary care and specialty roles, especially in rural and underserved areas where domestic recruitment often fails. These professionals typically enter the country through specific visa programs designed to address labor needs in high-skill sectors.
The impact is not limited to high-level clinical roles. The broader healthcare economy relies heavily on foreign-born workers in administrative, technical, and support positions. This includes laboratory technicians, radiologic technologists, and medical assistants. The diversity of the immigrant workforce allows the U.S. to maintain a complex, multi-layered system of care that can serve a culturally diverse patient population.
Why is the nursing profession particularly dependent on foreign-born workers?
The United States is currently grappling with what many experts call a “nursing crisis,” characterized by high burnout rates and an aging nursing workforce nearing retirement. To fill this gap, the healthcare industry has increasingly looked toward international recruitment. Many registered nurses (RNs) practicing in the U.S. today were educated abroad, often in countries such as the Philippines, India, and Nigeria.

This recruitment is driven by both domestic demand and international mobility. According to nursing industry reports, the shortage of nurses is projected to grow as the “Baby Boomer” generation requires more chronic disease management. Because the domestic pipeline of nursing students has not kept pace with this demand, hospitals often turn to international recruitment agencies to secure talent through specialized visas.
Foreign-born nurses often bring essential linguistic and cultural competencies that improve patient outcomes. In a country where language barriers can lead to medical errors, having a workforce that can communicate effectively with diverse patient populations is a clinical necessity. However, this reliance also creates a vulnerability; any significant shift in visa processing times or immigration restrictions can immediately impact hospital staffing levels and patient safety.
What role do immigrants play in long-term and home health care?
While much of the public discourse focuses on doctors and nurses, the most profound—and often least visible—impact of immigrant labor is in the direct care sector. This includes Certified Nursing Assistants (CNAs), home health aides, and personal care workers who facilitate long-term care (LTC) and home-based services.
The long-term care industry is arguably the most dependent on immigrant labor of any medical sub-sector. As the U.S. population ages, the demand for home-based care is skyrocketing. Many of the individuals providing this essential service are immigrants, including those who may be working under various legal statuses. These workers perform the foundational tasks of healthcare: assisting with mobility, medication management, and daily living activities.
The economic implications are significant. The “care economy,” fueled largely by immigrant labor, allows many American families to remain in the workforce because they have reliable, affordable care for elderly relatives. Without this workforce, the cost of formal institutional care would likely rise, and the burden of unpaid caregiving would fall disproportionately on domestic family members, particularly women.
What systemic barriers do immigrant healthcare workers encounter?
Despite their essential role, immigrant healthcare professionals face significant hurdles that can impede their ability to practice at the top of their licenses. These barriers are often structural, involving complex licensing requirements and restrictive immigration pathways.

One major obstacle is the process of medical credentialing. For foreign-trained physicians and nurses, navigating the various state boards to prove equivalency can be a multi-year, expensive, and exhausting process. Even after passing exams, many professionals find themselves in “underemployment,” working in roles below their actual skill level due to licensing delays or lack of recognition for their previous training.
Visa restrictions also create a sense of professional instability. Many healthcare workers rely on the H-1B or J-1 visa programs. The J-1 visa, which is common for medical residents, often carries a “home-country physical presence requirement,” meaning the physician must return to their home country for a period after their training unless they obtain a specific waiver. This requirement can disrupt the continuity of care in U.S. hospitals and complicates long-term workforce planning for medical institutions.
Furthermore, there is the issue of social and economic integration. Immigrant workers often face higher levels of scrutiny and may lack the same legal protections as domestic workers, particularly in the direct care and home health sectors. This vulnerability can lead to wage theft, unsafe working conditions, or difficulty accessing healthcare themselves.
How does immigration policy impact the stability of the medical workforce?
Because the healthcare workforce is so closely tied to immigration status, changes in federal policy have immediate consequences for clinical operations. Shifts in visa caps, changes to the “Green Card” backlog, or tighter border policies do not just affect migration patterns; they affect hospital staffing rosters.
When immigration policies become more restrictive, the cost of recruiting international talent rises. Hospitals must spend more on legal fees, recruitment agencies, and administrative overhead to secure foreign-born staff. In some cases, extreme policy shifts can lead to a “brain drain” effect, where highly skilled professionals choose to practice in countries with more stable and predictable immigration pathways, such as Canada or the United Kingdom.
Conversely, policies that streamline the path to permanent residency for healthcare workers have been shown to increase workforce stability. When clinicians have a clear, predictable path to legal permanent residency, they are more likely to commit to long-term roles in the communities they serve, rather than moving frequently to maintain visa compliance. This stability is crucial for rural healthcare providers who rely on a consistent staff to maintain essential services.
Comparison of Immigrant Roles in Healthcare
| Role Category | Primary Visa/Status Types | Key Sector Impact | Primary Barrier |
|---|---|---|---|
| Physicians (IMGs) | H-1B, J-1, O-1 | Hospitals, Specialty Care, Rural Clinics | Licensing & J-1 Waivers |
| Registered Nurses | H-1B, EB-3 | Acute Care, Hospitals, Surgery | Credentialing & State Boards |
| Direct Care Workers | Various (including undocumented) | Long-term Care, Home Health, Nursing Homes | Legal Status & Wage Protection |
Frequently Asked Questions
Do immigrant doctors provide better or worse care?
There is no clinical evidence to suggest that the quality of care is lower among immigrant doctors. In fact, many studies highlight that foreign-born physicians are vital in addressing health disparities in underserved and rural areas.
How does the nursing shortage affect patients?
Nursing shortages can lead to longer wait times, higher patient-to-nurse ratios, and increased risks of medical errors. The integration of foreign-born nurses is a primary strategy used by hospitals to mitigate these risks.
Can immigrant healthcare workers help with the aging population?
Yes. Immigrant workers provide a significant portion of the labor required for long-term care and home health services, which are increasingly necessary as the U.S. population ages.
What is a J-1 waiver?
A J-1 waiver is a legal mechanism that allows certain foreign-trained physicians to remain in the U.S. and bypass the requirement to return to their home country after their training, often by agreeing to work in an underserved area for a set period.
The next significant checkpoint regarding this issue will be the upcoming federal budget hearings, where healthcare staffing and immigration-related labor costs are expected to be discussed by congressional committees. We will continue to monitor these developments.
What are your thoughts on the role of immigration in healthcare? Do you believe current policies adequately support the medical workforce? Share your views in the comments below and share this article with your network.