
The Centers for Medicare & Medicaid Services (CMS) has initiated a new coverage model designed to provide Medicare Part D beneficiaries with access to GLP-1 receptor agonists for weight management. This “bridge” program marks a shift in how federal health plans handle medications like semaglutide, which have historically been excluded from Medicare coverage when prescribed specifically for weight loss due to statutory restrictions under the Social Security Act. According to the Centers for Medicare & Medicaid Services, the model aims to address the growing demand for obesity treatments among the aging population while navigating existing legal frameworks that prohibit Medicare from covering drugs solely for weight loss.
As a physician, I have observed the rising clinical importance of GLP-1 medications in treating obesity-related comorbidities. However, the intersection of medical innovation and federal policy remains complex. This bridge model is an attempt to reconcile the clinical needs of patients with the fiscal and legislative realities of the Medicare program. For millions of Americans, the question is not just about medical efficacy, but about the affordability and accessibility of these treatments within the current federal health infrastructure.
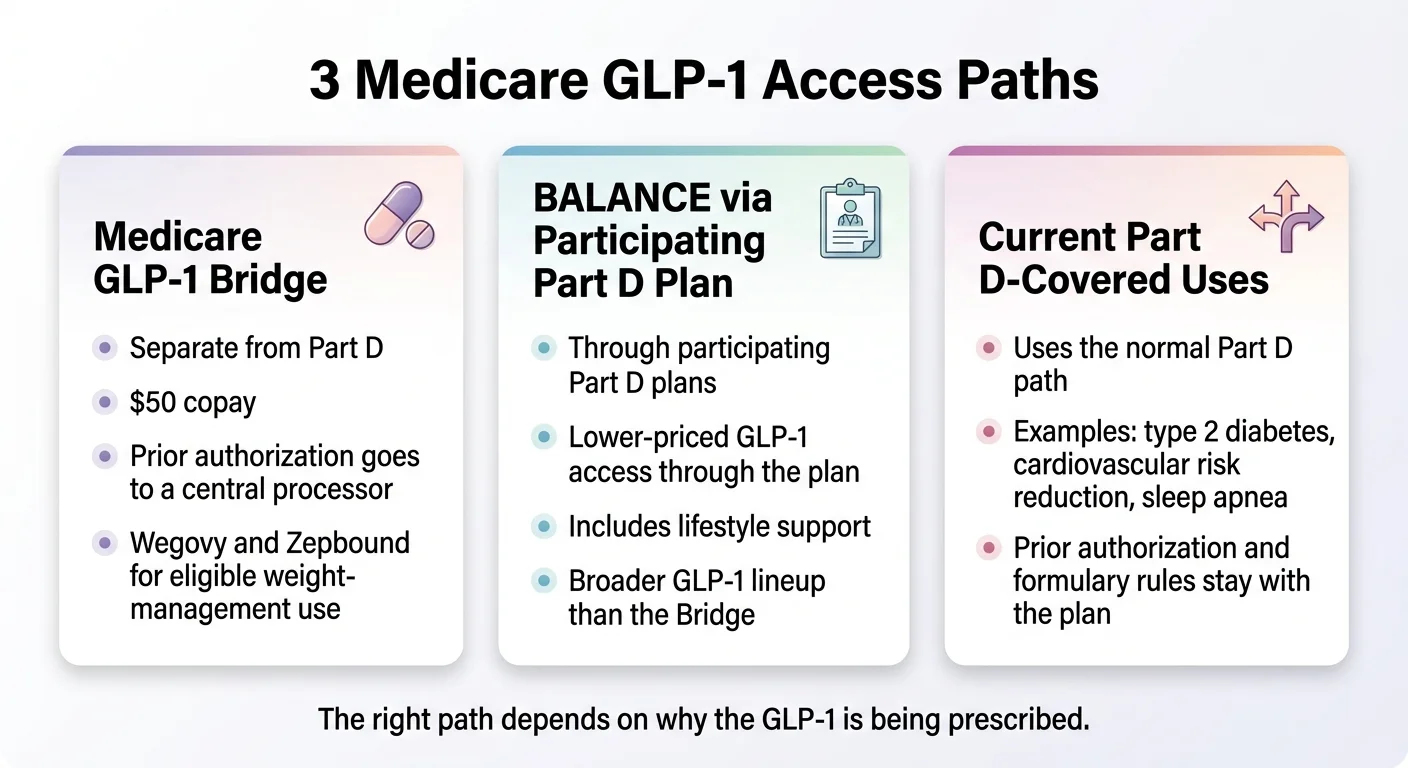
How the Bridge Model Functions
The core mechanism of the CMS bridge model involves creating a pathway that allows for the inclusion of GLP-1 medications within the Part D benefit structure under specific, controlled conditions. Historically, the Social Security Act has explicitly barred Medicare from covering weight-loss drugs. To bypass this, the new initiative utilizes demonstration authority, which allows the agency to test new payment and service delivery models on a limited scale.

Beneficiaries participating in the program may see changes in how their pharmacy benefits are processed. The model creates a framework where these medications are integrated into the existing Part D formulary, though access is strictly tied to clinical criteria. Officials have indicated that the program is designed to monitor health outcomes and cost-effectiveness, providing data that could inform future legislative changes regarding obesity drug coverage. The Department of Health and Human Services has emphasized that this is a temporary and targeted effort, rather than a permanent expansion of the underlying Medicare benefit.
Clinical Impact and Patient Eligibility
The clinical utility of GLP-1 agonists, such as Wegovy and Zepbound, extends beyond weight loss to the management of cardiovascular health and type 2 diabetes. While Medicare has previously covered these drugs for patients with type 2 diabetes, the “weight loss” indication remained an out-of-pocket expense for most. Under the new model, eligibility is expected to be determined by specific BMI thresholds and the presence of weight-related health conditions, such as hypertension or sleep apnea.

Physicians play a critical role in this process by ensuring that prescriptions meet the rigorous clinical guidelines established by the model. The Centers for Disease Control and Prevention notes that obesity affects over 40% of American adults, making this a significant public health challenge. By bridging the gap, CMS is attempting to reduce the long-term healthcare costs associated with obesity-related complications, such as heart disease and stroke, which are primary drivers of Medicare spending.
Financial Implications for Medicare
The financial sustainability of covering expensive weight-loss medications is a central concern for policymakers. The Congressional Budget Office (CBO) has previously analyzed the potential impact of expanding Medicare coverage to include anti-obesity drugs, highlighting the significant budgetary requirements associated with these high-cost biologics. According to the Congressional Budget Office, the net cost to the federal government depends heavily on the negotiated price of the drugs and the long-term reduction in other medical expenditures.
The bridge model incorporates cost-containment measures, including strict formulary management and potential manufacturer rebates. By limiting the scope of the program, CMS intends to gather the necessary data to understand whether the short-term cost of the medication is offset by a decrease in secondary medical interventions. This “evidence-based” approach is standard for CMS innovation models, which are often used to test hypotheses before a broader rollout is considered.
What Happens Next
The program is currently in its early implementation phase, with CMS expected to release additional guidance on enrollment and provider participation in the coming months. Beneficiaries are encouraged to monitor their specific Part D plan’s formulary updates and consult with their primary care providers regarding their eligibility. As of the latest update, no definitive timeline has been established for the expiration of this demonstration model, though it will be subject to periodic review by federal auditors and health policy analysts.
For patients seeking information, the most reliable resource remains the official Medicare.gov portal, which provides tools to check current coverage and plan options. As this policy evolves, further clarification from the agency regarding long-term coverage sustainability is expected. Readers are encouraged to share their experiences or questions in the comments section below, as we continue to track the impact of this policy on patient access to care.