
When a 22-year-old patient with cystic fibrosis received compassionate-use phage therapy for a chronic, drug-resistant Bordetella bronchialis infection, the treatment ultimately failed. Researchers later identified two key biological factors that may have undermined the therapy: pre-existing antibodies that cross-reacted with therapeutic phages and bacterial subpopulations with naturally reduced phage susceptibility, known as heteroresistance.
The case, published in Nature Medicine on April 24, 2026, highlights critical challenges in the clinical application of phage therapy, particularly for patients with long-term infections. Serum samples taken before treatment revealed the presence of antiphage immunity, suggesting the patient’s immune system had previously encountered similar viral structures. These antibodies were found to bind not only to endogenous prophages but too to the administered therapeutic phage, potentially neutralizing its antibacterial activity.
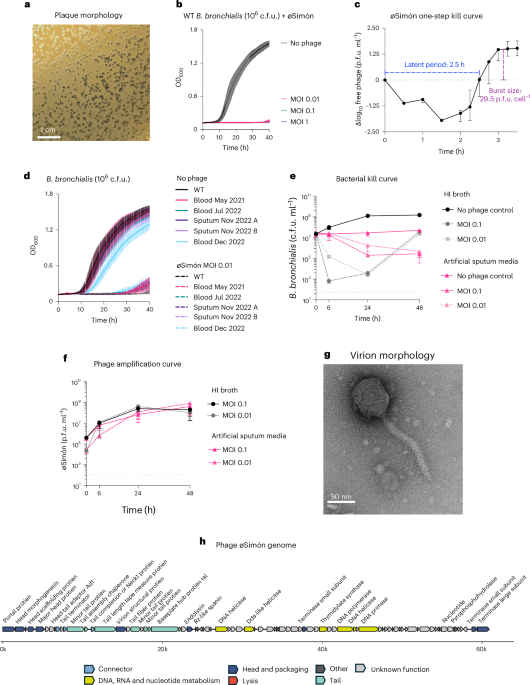
Phage therapy involves using viruses that specifically infect and kill bacteria to treat antibiotic-resistant infections. While promising, its success depends on multiple factors, including the phage’s ability to reach and replicate within the target bacterial population. In this case, researchers observed that the infecting Bordetella bronchialis strain harbored active prophages—viral genomes integrated into the bacterial chromosome—that could induce immune responses cross-reactive with the therapeutic phage.
bacterial heteroresistance was detected in the initial infection sample. This phenomenon describes subpopulations within a bacterial culture that exhibit transient or inherited reduced susceptibility to phages, even when the majority of the population remains sensitive. Such subpopulations can survive phage exposure and later repopulate, contributing to treatment failure despite an initially promising response.
The findings underscore the importance of screening patients for pre-existing antiphage immunity and assessing bacterial heteroresistance before initiating phage therapy, especially in chronic infections like those seen in cystic fibrosis. As noted in the study, future clinical protocols should evaluate immune history and microbial diversity across the entire treatment regimen to improve outcomes.
While phage therapy remains an investigational approach in most regulatory frameworks, cases like this provide essential insights into optimizing its use. Researchers emphasize that understanding the interplay between host immunity, bacterial genetics, and phage biology is crucial for advancing personalized antimicrobial strategies.
For updates on clinical phage therapy trials and guidance, readers may consult registries such as ClinicalTrials.gov or peer-reviewed journals tracking antimicrobial innovation.
Share your thoughts on the future of phage therapy in the comments below, and help spread awareness by sharing this article with others interested in medical advancements.