
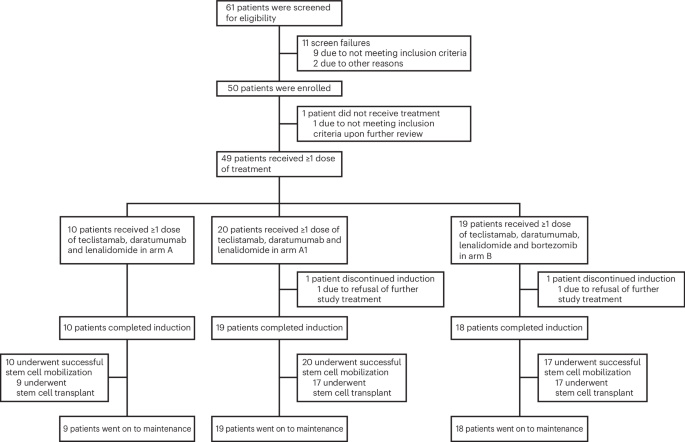
Early data from the phase 2 GMMG-HD10/DSMM-XX (MajesTEC-5) clinical trial indicates that incorporating the B-cell maturation antigen (BCMA)-directed bispecific antibody teclistamab into induction therapy for transplant-eligible, newly diagnosed multiple myeloma patients is both feasible and effective. According to preliminary findings, the combination of teclistamab with standard-of-care agents—specifically daratumumab and lenalidomide, administered with or without bortezomib—demonstrated a toxicity profile consistent with existing bispecific T-cell engager (BiTE) regimens while eliciting deep and encouraging therapeutic responses.
As a physician monitoring advancements in hematologic oncology, I view these results as a significant indicator of how immunotherapy is shifting toward earlier lines of treatment. Multiple myeloma, a cancer of the plasma cells, remains a complex condition where the goal of initial induction therapy is to achieve the deepest possible remission before patients undergo autologous stem cell transplantation. By moving potent bispecific therapies like teclistamab into the induction phase, researchers aim to improve long-term outcomes for patients who are otherwise fit enough for intensive treatment protocols.
Understanding Teclistamab in Frontline Settings
Teclistamab is a bispecific T-cell engager designed to bridge T-cells to myeloma cells by targeting BCMA on the tumor surface and CD3 on the T-cells, effectively hijacking the immune system to destroy malignant cells. While the U.S. Food and Drug Administration (FDA) initially granted accelerated approval for teclistamab in 2022 for the treatment of relapsed or refractory multiple myeloma, its utility in the frontline setting—specifically for those who are transplant-eligible—has been the subject of intensive investigation, as noted by the U.S. Food and Drug Administration.

The MajesTEC-5 trial aims to determine if the addition of this immunotherapy can deepen the response rates observed with conventional triplet or quadruplet therapies. In current clinical practice, the standard of care for transplant-eligible patients typically involves a combination of a proteasome inhibitor (such as bortezomib), an immunomodulatory drug (such as lenalidomide), and a corticosteroid, often supplemented with a monoclonal antibody like daratumumab. The integration of teclistamab into this sequence represents a strategic effort to eliminate minimal residual disease (MRD) more effectively than traditional chemotherapy-based backbones alone.
Clinical Efficacy and Safety Profiles
The primary concern with introducing bispecific antibodies into induction therapy is the potential for additive toxicities, particularly cytokine release syndrome (CRS) and neurotoxicity. According to the Multiple Myeloma Research Foundation, managing these immune-mediated side effects requires specialized clinical oversight. Data from the MajesTEC-5 study suggests that when administered in a controlled trial environment, the safety profile of the teclistamab-based combination did not exceed the expected thresholds for patients receiving intensive myeloma induction, providing a rationale for further investigation in larger, phase 3 cohorts.
Deep response rates, measured by the ability to achieve a complete response or better, are critical predictors of progression-free survival in myeloma. The trial investigators observed that the combination regimen was able to induce these deep responses in a high proportion of patients. This is consistent with the broader trend in oncology where bispecifics are being evaluated for their potential to provide durable control early in the disease trajectory, potentially reducing the reliance on subsequent lines of salvage therapy.
The Path Forward for Transplant-Eligible Patients
For patients and clinicians, the question remains how these results will influence future treatment guidelines. Currently, the standard of care remains anchored in established triplet and quadruplet regimens, and the use of teclistamab remains largely confined to patients who have exhausted at least four prior lines of therapy, according to the European Medicines Agency. The MajesTEC-5 trial is a necessary step in generating the high-quality evidence required to support a move toward earlier intervention.

Researchers are expected to provide further updates on the durability of these responses and long-term safety data as the trial progresses. These findings are essential for determining whether the clinical benefit of using teclistamab upfront justifies the logistical requirements of administration and the management of immune-related adverse events. As data from phase 2 trials matures, the oncology community will look for confirmation that this approach can be safely and effectively scaled to a broader patient population.
The next scheduled updates for the GMMG-HD10/DSMM-XX trial are expected to be presented at upcoming international hematology conferences, where investigators will report on extended follow-up periods. Readers interested in the latest developments in multiple myeloma treatment are encouraged to consult their primary oncology team or visit official registries, such as ClinicalTrials.gov, for information on ongoing study enrollment and site availability. Please share your thoughts on the evolution of frontline myeloma therapy in the comments section below.