A Phase 1 clinical trial has reported that the experimental combination of englumafusp alfa and glofitamab demonstrates an acceptable safety profile and preliminary clinical efficacy in patients with relapsed or refractory aggressive B-cell non-Hodgkin lymphoma. This therapeutic approach utilizes englumafusp alfa, a CD19–4-1BBL co-stimulatory molecule, alongside the established bispecific antibody glofitamab, according to data published in Nature Medicine. The study provides mechanistic evidence supporting the rationale for combining these agents to enhance immune-mediated anti-tumor activity in patients who have exhausted standard treatment options.
Aggressive B-cell non-Hodgkin lymphoma, including subtypes such as diffuse large B-cell lymphoma (DLBCL), remains a significant clinical challenge when the disease fails to respond to initial therapies or recurs. The combination of englumafusp alfa and glofitamab is designed to address this by leveraging the body’s own immune system. Glofitamab, which is already approved in several jurisdictions for specific lymphoma indications, functions as a T-cell engaging bispecific antibody. By adding englumafusp alfa, researchers aim to provide a secondary “co-stimulatory” signal to T-cells, potentially overcoming the exhaustion or insufficient activation often seen in the tumor microenvironment.
Clinical Trial Design and Safety Signals
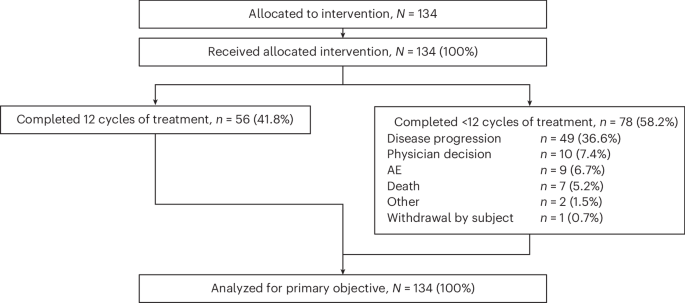
The Phase 1 trial was primarily structured to determine the safety, tolerability, and recommended dosage for the combination therapy. In oncology research, Phase 1 studies are critical for identifying dose-limiting toxicities and establishing a therapeutic window before efficacy is evaluated in larger, randomized Phase 2 or 3 trials. According to the study findings, the combination was generally well-tolerated, with safety signals consistent with the known profiles of bispecific antibodies and immunotherapy agents. Common adverse events in such trials typically include cytokine release syndrome (CRS) or neurological toxicities, though the specific incidence rates for this combination are detailed in the full clinical report available through the Nature Medicine digital archive.
The mechanistic rationale for this dual-agent approach is rooted in the biology of T-cell activation. While glofitamab binds to both CD3 on T-cells and CD20 on B-cells to bring them into proximity, englumafusp alfa acts on the CD19 receptor. By engaging CD19 and providing 4-1BBL signaling, the therapy seeks to amplify the T-cell response. This dual-targeted strategy is intended to prevent the tumor from evading the immune system by modulating the co-stimulatory pathways that sustain long-term T-cell function.
Therapeutic Implications for Refractory Lymphoma
For patients with relapsed or refractory aggressive B-cell non-Hodgkin lymphoma, the standard of care has evolved rapidly with the introduction of chimeric antigen receptor (CAR) T-cell therapies and bispecific antibodies. However, not all patients achieve durable remissions. The focus of this research is to identify whether combinations can offer a viable alternative for those who do not qualify for or have failed CAR T-cell therapy. The encouraging preliminary clinical responses observed in this trial suggest that the combination of englumafusp alfa and glofitamab may represent a meaningful addition to the hematologic oncology toolkit.
Further investigation is required to determine the durability of these responses and how the combination performs across broader patient populations. Clinical trials for hematological malignancies are strictly regulated, and updates regarding the progression of this study, including future site recruitment and patient eligibility, are typically tracked through the U.S. National Library of Medicine clinical trials database.
Next Steps in Clinical Development
The next phase of development for this therapy will likely involve larger cohorts to confirm the response rates and optimize the dosing schedule. Researchers will monitor for long-term safety signals and evaluate whether the combination provides a survival benefit compared to existing monotherapies. As with all clinical research, definitive conclusions regarding the efficacy of this combination must wait for the completion of subsequent trial phases.
Patients and providers seeking information on current treatment options or trial participation should consult with their hematologist or oncologist. Official updates regarding the regulatory status of new lymphoma therapies are managed by agencies such as the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA). Readers are encouraged to share their thoughts on these advancements in blood cancer treatment or post questions regarding the latest findings in the comments section below.
Worth a look