Growth-plate pain, clinically known as apophysitis, is a common condition among active adolescents during puberty, typically manifesting as localized discomfort in the hips, knees, or feet. While the condition can cause children to limp or reduce their physical activity, evidence regarding the efficacy of various medical and physical interventions remains largely uncertain. Most cases are self-limiting and resolve naturally as the child’s growth plates close, according to research synthesized by the Cochrane Library.
It is essential to understand that while many treatments—ranging from orthotics to physical therapy—are commonly prescribed, the scientific consensus on their ability to accelerate healing or reduce pain is currently limited by the small scale and design constraints of existing clinical trials.
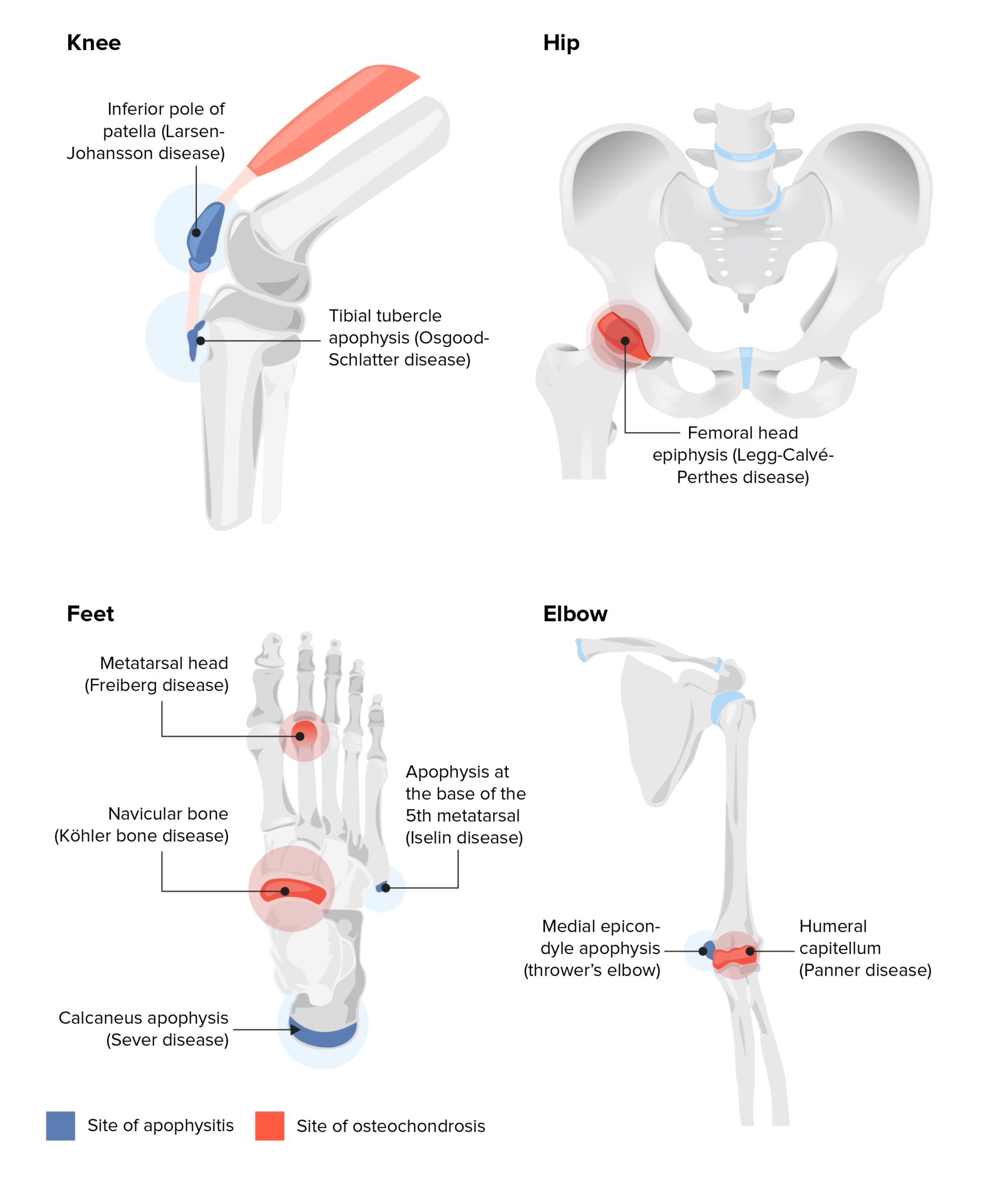
Understanding Apophysitis and Its Causes
Apophysitis occurs when the growth plates, or apophyses, become irritated due to repetitive stress rather than a single acute injury. This mechanical stress leads to inflammation and pain at the site of the growth plate. Common presentations include heel pain, often referred to as Sever’s disease, or pain at the front of the knee, known as Osgood-Schlatter disease.
Because the condition is fundamentally linked to the natural process of skeletal maturation, it is often difficult for clinicians to distinguish between the effects of a specific treatment and the natural recovery that occurs as the growth plate matures. According to the Cochrane review, which analyzed 10 studies involving 654 children, there is a lack of high-certainty evidence to suggest that one specific treatment is superior to another for managing pain or improving physical function.
Evaluating Current Treatment Options
Healthcare professionals, including general practitioners, physiotherapists, and podiatrists, employ a variety of strategies to manage symptoms. However, the quality of evidence supporting these interventions is frequently undermined by small sample sizes and study designs where participants are aware of the treatment they are receiving, which may introduce bias into the reporting of pain reduction.
Clinical trials have examined several common approaches:
- Medication: Studies comparing anti-inflammatory medications like dexamethasone to placebos have failed to provide clear evidence that these drugs effectively reduce pain or improve a child’s ability to return to sports.
- Orthotics and Footwear: Research comparing foot orthoses to simple heel lifts suggests that there is likely little to no difference in outcomes regarding short-term pain relief or physical function.
- Taping and Bracing: The use of Kinesio tape and various straps has been investigated, but current data is insufficient to definitively state whether these methods offer benefits over a placebo.
In many of these studies, the lack of reported data regarding participant withdrawal due to adverse effects makes it challenging to draw firm conclusions about the safety and tolerability of these interventions for long-term use.
Limitations in Clinical Research
One of the primary challenges in treating apophysitis is the demographic bias present in existing research. Most studies have focused on highly active children, with a disproportionate number of male participants. While it is generally assumed that the condition does not affect boys and girls differently, the current body of evidence may not accurately reflect the experiences of less active children or a broader, more diverse population.
Furthermore, because the condition often improves on its own over time, the “placebo effect” or the natural healing trajectory of the growth plate can make it appear as though an intervention is effective when it may not be. As of the most recent evidence update on January 4, 2025, there is no standardized, gold-standard treatment that has been proven to consistently shorten the duration of these injuries.
Practical Guidance for Families
For parents and young athletes, the most important takeaway is that apophysitis is typically a temporary, non-surgical condition. While pain can be disruptive, it does not usually cause long-term harm.
While you may be offered various strapping, cushioning, or physical therapy exercises, it is reasonable to discuss the uncertainty of these treatments with your provider.
As researchers continue to conduct larger, more robust clinical trials, our understanding of these injuries will continue to evolve. For now, patience and symptom-based management remain the clinical standard. If you have questions about your child’s specific symptoms or need to discuss a treatment plan, please consult your primary care physician or a pediatric sports medicine specialist. We encourage you to share your experiences or questions in the comments below.
Keep reading