Public health experts are increasingly questioning the universal expansion of breast cancer screening programs, arguing that the medical risks of overdiagnosis often outweigh the potential survival benefits for certain patient groups. Recent evaluations suggest that shifting away from the traditional “screening saves lives” narrative is necessary to better account for the clinical complexities and unintended consequences associated with mass mammography programs.
The debate centers on the balance between early detection and the phenomenon of overdiagnosis—where screening identifies non-lethal tumors that would never have caused symptoms or death in a patient’s lifetime. According to the Belgian Health Care Knowledge Centre (KCE), which provides evidence-based policy advice, expanding screening programs to include broader demographic groups does not inherently lead to better health outcomes and may, in many cases, introduce unnecessary medical interventions.
Understanding the Risks of Overdiagnosis
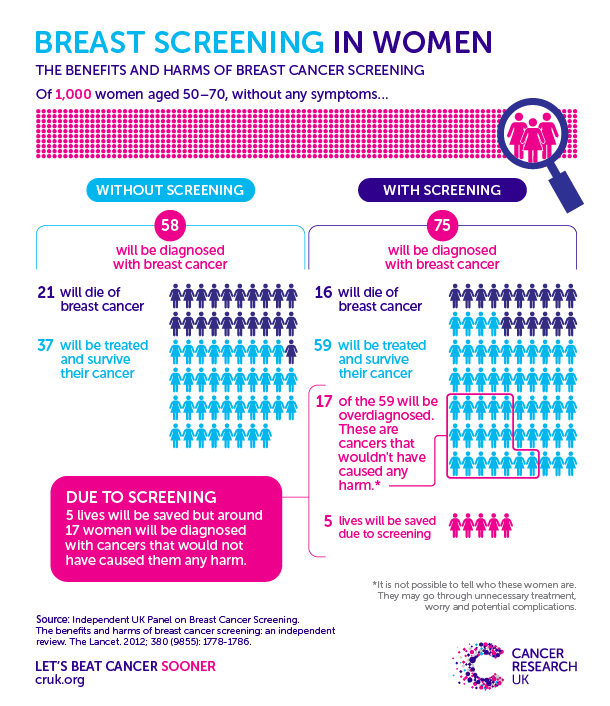
Overdiagnosis occurs when a screening test detects a malignancy that is either slow-growing or biologically indolent. Because it is often impossible to distinguish these “harmless” tumors from those that are aggressive, clinicians frequently proceed with standard treatments, including surgery, radiation, or chemotherapy. This exposes patients to significant physical and psychological side effects without providing a genuine clinical benefit.
Research indicates that for every life saved through early detection, a larger number of women may undergo unnecessary treatments for cancers that would not have progressed. The European Association of Science Editors and various public health bodies emphasize that informed decision-making—rather than blanket population-wide testing—should be the priority. This approach respects patient autonomy by ensuring individuals understand the limitations and potential harms of screening before choosing to participate.
Why Universal Expansion Faces Pushback
The call to reconsider the expansion of screening programs is rooted in the “harm-benefit ratio.” Critics of universal expansion point out that as screening protocols become more inclusive, the number of false positives increases. False positives trigger a cascade of secondary tests, including biopsies and additional imaging, which cause significant patient anxiety and contribute to the rising costs of healthcare systems.
In many regions, public health authorities are moving toward more personalized risk-assessment models. Instead of a one-size-fits-all approach based primarily on age, experts suggest that screening should be tailored to an individual’s specific risk profile, which includes factors like family history, genetic predispositions, and breast density. This shift aims to focus resources on the groups where the clinical impact of screening is most profound, while reducing the burden of over-screening on the general population.
Shifting the Public Health Narrative
For decades, campaigns have utilized the slogan “screening saves lives” to encourage participation. However, modern medical communications are increasingly nuanced. Experts argue that this slogan is an oversimplification that masks the reality of the screening process. By moving away from deterministic language, health services aim to foster a more transparent dialogue between physicians and patients.
The World Health Organization notes that while early detection remains a pillar of cancer control, it must be integrated into a comprehensive health system that includes timely diagnosis and high-quality treatment. The current movement among experts is not to abolish screening, but to refine its application. This means prioritizing high-risk groups and ensuring that the decision to be screened is supported by clear, evidence-based data regarding the specific risks and benefits for that individual.
Next Steps for Policy and Practice
Healthcare policy remains in a state of transition as institutions digest these findings. Future updates to national screening guidelines are expected to emphasize the importance of shared decision-making. Patients are encouraged to consult their primary care physicians or oncologists to discuss whether routine screening is appropriate based on their unique health history and current clinical evidence. Official updates regarding screening recommendations are typically published by national health ministries or health technology assessment agencies.
As the conversation around breast cancer screening continues to evolve, your input and experiences are valuable. If you have questions about current screening protocols or have encountered challenges in navigating these clinical decisions, feel free to share your perspectives or join the discussion in the comments section below.