Aoife M. Doyle
2026-02-02 00:00:00
We followed STROBE guidelines for the reporting of cohort studies (Supplementary Table 7).
Study location
Zimbabwe was selected to participate in this study after formative research during which stakeholders indicated strong support for check-ups, as they would address an unmet need for healthcare among the adolescent population18. In addition, the 2018 Zimbabwean School Health Policy provides a policy framework for the provision of comprehensive school health programming46 and the implementation of health education and promotion. This initial Y-Check research is focusing on urban areas where there is a high number of adolescents and anticipated high levels of risk behaviors—for example, lack of exercise and substance use. Chitungwiza, with a population of 271,000, is the third-largest urban area in Zimbabwe.
Intervention design
We developed the intervention through expert consultation, literature review, qualitative interviews and co-design workshops with adolescents and key adults in their lives, policymakers, programmers and healthcare workers18,26.
In 2020, formative work on the development of Y-Check in Zimbabwe involved a desk review of relevant epidemiological and health program data, participatory workshops with adolescents and parents and in-depth interviews with key informants, including policymakers, programmers and healthcare workers. The introduction of routine health check-ups was strongly supported by stakeholders, and they shared their preferences for check-up implementation format and content18.
In this phase of research (2021–2025), to further design the intervention content, we reviewed relevant literature and established health condition-specific technical advisory groups comprising local and international experts to advise on screening, treatment and referral protocols for each condition. Stakeholder engagement activities started in November 2021 and involved meetings with key Ministry of Health and Childcare and Ministry of Primary and Secondary Education personnel, the formation of a Youth Advisory Group and meetings with head teachers and class teachers in study schools. We also visited health facilities and met with service providers to negotiate the setup of referral pathways.
Between December 2021 and October 2022, we used a person-based design approach with adolescents (10–19 years old) to plan, test and refine the screening tools for the health and well-being check-ups26. Five workshops and cognitive interviewing sessions with adolescents led to modifications in the check-up content, screening tool wording and the appearance and functioning of the bespoke screening app. Additional input was received from the Youth Advisory Group and expert adolescent health and well-being stakeholders.
In June 2022, a pilot study was conducted with 171 adolescents recruited from two primary schools, two secondary schools and two community venues in Chitungwiza. After the pilot study, the check-up visit was further adapted based on the pilot screening results and process evaluation feedback from the adolescents, school staff and parents/guardians (Y-Check pilot study report available online at https://www.thruzim.org/adolescent-health-1/y-check).
Evaluation tool design
The development of the evaluation questionnaire followed similar procedures to the intervention design and included literature review and expert consultation to identify the most appropriate questionnaire content, followed by translation into Shona and back-translation into English and pre-testing and piloting with adolescents to ensure acceptable wording and length. Existing questionnaires, such as the Global School-based Student Health Survey (https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/global-school-based-student-health-survey) and Demographic Health Surveys (https://www.dhsprogram.com/), informed questions on health-related knowledge, intentions and behaviors. Standard tools were used for alcohol and substance use (CRAFFT 2.1 (https://crafft.org/)), self-esteem49 and health-related quality of life (CHU9D)50. In addition, a co-design workshop with 16 adolescents explored the outcomes that are important to adolescents and led to the following youth-centered evaluation outcome: ‘Perception of the importance of getting their health checked’.
Study design and participants
This intervention study, with a mixed-method process evaluation, was conducted in four primary schools, two secondary schools and two community venues. To align with the WHO recommendations of one check-up in early adolescence and one check-up in older adolescence13, the intervention was delivered to one year group in each school: Grade 5 in primary school and Form 3 in secondary school. To maximize the feasibility of the study and diversity of participants, we worked with the Ministry of Primary and Secondary Education in Chitungwiza to select schools that fulfilled the following inclusion criteria: enrollment of 200–500 Grade 5 or Form 3 students per school year, students from various socioeconomic backgrounds, and schools likely to be supportive of health interventions but with no active or recent health programs.
Individual inclusion criteria
Primary schools: age 10–14 years, enrolled in Grade 5 in 2022, received parental consent and provided assent. Secondary schools: age 15–19 years, enrolled in Form 3 in 2022, received parental consent and provided assent. Community venues: age 16–19 years, living in a predefined catchment area near the community venue and provided their own informed consent.
Participant recruitment and informed assent/consent
Within the selected schools, lists of potentially eligible participants were taken from school enrollment registers. Parents/guardians and students were invited to information meetings at the schools, at the end of which they were invited to sign the consent forms. They also had the option to take the forms home for further review before deciding whether to sign them. Students could participate in only the check-up visit or in both the check-up visit and the research cohort. Completed forms were returned to the study team through the schools. Prior to any study procedures, adolescents with parent/guardian consent gave their written assent. In the community venues, catchment areas surrounding each venue were clearly demarcated. Mobilizers identified adolescents aged 16–19 years who were interested in participating and accompanied them to the community venues where they were screened for eligibility and, if eligible, consented to the study.
Procedures
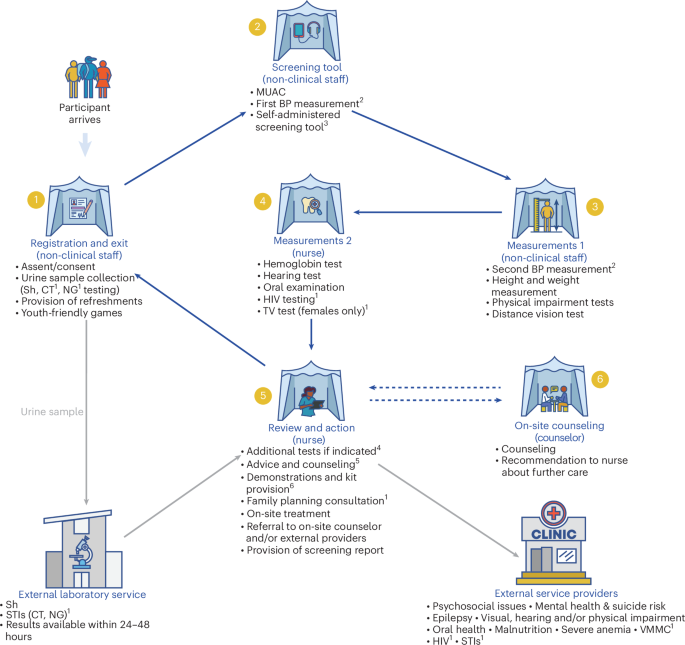
The check-up took place in tents on the school grounds or at community venues and consisted of registration, an audio/computer-assisted self-completion screening questionnaire, physical assessments and nurse review (Fig. 1). Check-up data were collected on tablet computers using a bespoke, youth-friendly digital application. Y-Check staff were available to assist with tablet use and comprehension of the questions and administered the questions when necessary. In-built algorithms used the data to generate ‘warning flags’ (green, no concern; orange, some concern; red, considerable concern) for health conditions and risk behaviors. Orange and red warning flags were then reviewed by a nurse, who either discussed with or examined the adolescent to determine if further action was needed. When no issue was present, the nurse marked an orange or red warning flag as a ‘false warning flag’. Potential actions included providing information, treatment, onward referral to an in-house counselor or referral to external service providers with whom referral arrangements were negotiated in advance. Where feasible, participants were referred to government service providers; otherwise, they were referred to private for-profit or not-for-profit service providers. All adolescents received a printed screening report at the end of their visit, and those requiring referral to an external service provider were provided with a paper referral form. The issues screened for and potential actions taken are described in Supplementary Table 4. The nurse also applied fluoride gel to all participants’ teeth to prevent cavities and provided general health information and advice, including proper tooth and gum brushing techniques, good sleep habits, physical activity and maintaining a healthy balanced diet. Physical games were available to the adolescents while they were waiting, and all participants received a healthy food snack, toothbrush and toothpaste. In addition, females received reusable menstrual hygiene pads, two pairs of underwear, a bar of soap and information on menstrual health.
Attendance at the first referral appointment was recorded through a paper referral form that the participant took to the referral appointment. Prior to the start of the intervention, service providers were orientated to the Y-Check study and completion of the paper referral form. Memoranda of understanding (MoU) were signed with providers that outlined the services that would be provided and any associated costs. Incidental findings not included in the MoU would not be covered by the study. The check-up visit and all clinical costs related to the first referral services were provided free of charge to the participants as long as this occurred within 6 months of the check-up. However, where the participant had been non-contactable, their referral costs were covered if they were then contacted during the follow-up visit and attended the referral appointment (up to 10 months after check-up). Some referral facilities were in Chitungwiza, but other services were available only in Harare, 25 km away. Group transport for adolescents and their parent or guardian was provided for referrals to Harare but not within Chitungwiza.
Confidentiality and information sharing
All medical information was deidentified and recorded using a unique study identification number. Identifying information, such as names, addresses and phone numbers, was recorded in a registration book that was stored in a locked container when not in use. Adolescents received their screening results verbally from the nurse. They also received a letter with results for them to take home to their parent/guardian. Medical information was not shared with other students or teachers. However, in instances where a participant was identified as being suicidal and required emergency care, the school health coordinator and school head teacher were informed. Decisions around who would accompany the young person to the referral service took place in consultation with school staff, parents/guardians and/or trusted adults who had been nominated by older adolescents at community venues during registration.
Outcome evaluation
At baseline, just prior to the health check-up, data on sociodemographic variables and some of the evaluation outcomes were collected using an adolescent self-completion structured questionnaire programmed in Open Data Kit (ODK). Follow-up questionnaires and measurements were conducted 5–7 months after intervention. The follow-ups were done at the same schools and community venues, with participants invited through schools and via phone calls by the community mobilizers. If the participant’s phone number was unreachable, SMS messages were sent requesting that the participant get in touch as soon as they received the message. Where participants were unreachable over the phone, up to three home visit attempts were made before determining them as lost to follow-up. Participants who had relocated to other parts of the country were offered bus fare reimbursement for them to return for the follow-up visit.
The primary outcome was the proportion of participants who screened positive for at least one issue (condition or behavior) and received appropriate on-the-spot care and/or completed appropriate referrals for all identified issues by the time of the follow-up. The list of health issues included in the primary outcome is provided in Supplementary Table 4. Completing appropriate referral was defined as attending at least one referral visit for each issue identified, which was measured by retrieving the referral form from the service provider. Participants who were already receiving care for their issue(s) and who did not require further intervention were considered to have received appropriate on-the-spot care. Secondary implementation outcomes included the proportion of participants who screened positive for individual issues and received appropriate on-the-spot care and/or completed appropriate referrals by the time of the follow-up visit as well as the yield of untreated conditions and the prevalence of risk behaviors. We also evaluated the status at follow-up of the following previously diagnosed conditions: STI symptoms, STI test positive, symptoms suggestive of depression and/or anxiety, suicide risk, epilepsy and visual and hearing impairment (Supplementary Table 5).
Other implementation outcomes were assessed through a mixed-methods process evaluation, guided by the Medical Research Council process evaluation framework51. We adapted Proctor’s Implementation Outcomes Framework52 to focus on five of the implementation outcomes: acceptability, adoption, appropriateness, feasibility and fidelity.
Secondary individual outcomes, mapped onto the Theory of Change15, were health-related knowledge (measured using an six/eight-item quiz); intention to adopt a healthy behavior (avoid drugs and alcohol and be more active); agency to make decisions about health; health-related risk and protective behaviors (sweetened drink consumption, fruit consumption, support for mental health, sleep, physical activity, substance and alcohol use, smoking, tooth brushing, sexual risk behavior and HIV testing); engagement with health services in the past 4 months; self-esteem (Rosenberg self-esteem scale); health-related quality of life (CHU9D) and life satisfaction as a measure of subjective well-being; clinical outcomes (anemia, thinness (body mass index (BMI) for age and sex (z-score less than −2 s.d.)) and obesity (BMI for age and sex (z-score greater than +2 s.d.)); educational outcomes (days missed in the past month due to illness or menstruation, perception of school results, impaired performance or reduced participation due to ill-health); and perception of the importance of getting health checked (youth-centered outcome) (Supplementary Table 5).
Sample size
The sample size calculations assumed that 30% of participants would screen positive for at least one issue (condition/behavior) and that 75% of those who screened positive would be correctly managed. With 500 participants in total, and 150 screening positive for at least one issue in each of the four age/sex groups, the 95% confidence interval for the primary outcome of correct management would be 68.0−82.0%.
Process evaluation
Process evaluation data were collected using diverse qualitative and quantitative methods (Supplementary Table 6). Qualitative data were generated by S.M., F.R.K., C.A.N. and C.R.S.M.-Y., who were distinct from the intervention team but collaborated closely with them throughout.
Observations
Non-participant observations were conducted of (1) the Y-Check screening, (2) referral services provision and (3) intervention team biweekly debrief meetings. All observations were conducted with the awareness of participants and service providers. Observations of screening and referral services centered on interactions of intervention staff, adolescents and service providers during the provision and receiving of services. Informal conversations with intervention staff, participants and service providers were also conducted during observation visits, and, in some cases, data generated during observations were explored in more detail within in-depth interviews. Observations of biweekly team debriefing meetings were conducted to understand experiences, challenges and adaptations in intervention delivery. Observations were guided by semi-structured observation guides. Detailed field notes and minutes were captured during observations and written up after each observation. The observation notes for each observation included a section on reflection, which included specific reflections on ‘How do you think your presence influenced what happened during the observation?’
In-depth interviews
Qualitative interviews were conducted with adolescents who received the Y-Check intervention (n = 9), adolescents who were referred (n = 10), service providers (n = 5), intervention staff (n = 7) and school authorities (n = 6) using the participants’ preferred language (English or Shona). A range of participants was purposively selected, based on the following characteristics: location of intervention (that is, primary school, secondary school or community), sex and age. In-depth interviews were guided by topic guides that explored the acceptability, appropriateness, feasibility, fidelity and adoption of the Y-Check intervention. All interviews were conducted in a private setting (at school or in a participantʼs home), were audio recorded, transcribed and, when necessary, translated into English and lasted around 45–60 minutes.
Participatory workshops
Thirteen participatory workshops (8–10 participants) were held separately with adolescents, their parents and teachers within 3 months of the initial check-up. These included adolescents who participated in the Y-Check intervention (n = 5 workshops), adolescents who did not participate in the intervention (n = 4 workshops), parents of adolescents who participated in the Y-Check intervention (n = 2 workshops) and parents of adolescents who did not participate in the intervention (n = 2 workshops). All participatory workshops were guided by semi-structured guides, covering topics around (non)acceptability, appropriateness, feasibility and sustainability of the intervention. Additionally, workshops with parents covered topics on how parental support and consent might be improved. All workshops were facilitated in the participants’ preferred language (English or Shona), were recorded and lasted around 2−3 hours each.
There was only one major deviation from the published protocol15. The original design proposed a first follow-up visit after 4 months with a second follow-up at 12 months15, but, due to implementation delays, the first follow-up visits occurred 5–7 months after the intervention. As a result, the planned second follow-up at 12 months did not take place as it was considered too close to the first follow-up to provide substantial additional value.
Cost analysis
We followed the International Decision Support Initiative reference case to guide the planning, conduct and reporting of the economic evaluation of Y-Check (https://idsihealth.org/resource-items/idsi-reference-case-for-economic-evaluation/). In this paper, we report analysis from the provider’s perspective. The intervention ran for 18 months and included a start-up phase (intervention development and piloting, from September 2021 to September 2022) and an implementation phase (from October 2022 to March 2023). Costs associated with referrals to external service providers that took place between October 2022 and September 2023 were included.
A combination of top-down and ingredients-based costing approaches was used to identify, measure and value resources used for delivering the whole package and for each component/activity. Resources used were identified and measured using process evaluation data, document review and financial and accounting records. Staff time spent on each service (that is, time spent testing or treating per condition/risk behavior) was collected through interviews and ODK timestamps. Both financial and economic costs were considered. All research costs, such as monitoring and evaluation, were excluded. Expenses were incurred either in US$ or the now-obsolete Zimbabwean Dollar (ZWL). All costs paid in ZWL were converted to US$ at the spot rate of the date of the transaction. Costs are presented in US$ 2023 and are discounted at 3% as the international standard.
The Y-Check intervention costs were analyzed using an adapted Excel-based costing tool53. We estimated the total cost of setting up and implementing the Y-Check intervention in school and community settings, including testing, on-the-spot care, referral and administrative/management costs. To understand the costs around implementing the check-up itself, we also estimated:
-
1.
The cost per adolescent reached, which was calculated as the total cost of implementing the Y-Check intervention (that is, screening and treating the participants), excluding referral costs and indirect or support costs (for example, administrative or support activities not directly associated with delivery), divided by the total number of adolescents who received Y-Check.
-
2.
The total cost to screen, treat and/or refer participants, which was calculated as the total cost of implementing Y-Check, excluding indirect or support costs (for example, administrative or support activities not directly associated with delivery), divided by the number of adolescents who received Y-Check.
Statistical analysis
Analysis was conducted in Stata 18. The proportion of potentially eligible adolescents aged 16–17 years in community settings was estimated using population census data. Participants’ baseline sociodemographic characteristics were used to compare the community-level and school-level characteristics of study communities and schools. Sociodemographic characteristics of participants at baseline and follow-up were compared.
The screening test results, services delivered on the spot and referrals made and completed were collated and reported by sex and age group and/or location. Survey implementation variables were described at each timepoint.
The primary outcome and secondary outcomes measured at a single timepoint were estimated as a proportion with a 95% confidence interval for four age/sex groups: 10−14-year-old males, 10–14-year-old females, 15–19-year-old males and 15–19-year-old females. Preplanned sensitivity analyses for the primary outcome included (1) adjustments to the definition of ‘screen positive’ to account for incorrect app algorithms; (2) limiting the outcome to receipt of on-the-spot care only; (3) using self-reports as well as documented attendance as evidence of attendance at referral appointments; and (4) restricting referral attendance to only those who attended within 4 months. Two additional post hoc sensitivity analyses were conducted: (1) restricting the analysis to issues applicable to all sex and age groups and (2) excluding issues that were previously diagnosed and did not require further management.
For conditions where follow-up clinical outcomes were measured only among those who screened positive at baseline, the prevalence of the condition at follow-up was calculated, with a 95% confidence interval. For outcomes that were measured at two timepoints, a pre−post analysis was conducted to compare differences in measures between the two timepoints. The percentage difference in prevalence of each outcome was calculated with 95% confidence intervals. Prevalence ratios and 95% confidence intervals were estimated using a mixed-effects population-averaged generalized linear model with Bernoulli distribution and logit link function, adjusting for school/community as a fixed effect. The Wald test was used to estimate P values.
The proportion of missing values for individual conditions was reported as a percentage of those who were eligible to be assessed for the condition. Baseline information from clients lost to follow-up was retained in relevant analyses.
Qualitative analysis
Analysis of the implementation of Y-Check was guided by Proctor’s Implementation Outcomes Framework52, focusing on the five implementation outcome domains that are most relevant to this phase of Y-Check research (that is, Feasibility, Fidelity, Adoption, Acceptability and Appropriateness). The qualitative and quantitative data that were relevant to each domain were identified from the full dataset. Qualitative data were manually analyzed thematically and inductively. We composed an analytical memo for each domain and then subsequently refined this iteratively by triangulating with data across different sources and grouping the data thematically. This process of analytical refinement was guided by regular discussions within the process evaluation team to discuss key emerging sub-themes.
Further details on the intervention and its evaluation are provided in the published study protocol15.
Inclusion and ethics statement
This study was designed through a longstanding partnership among the Biomedical Research and Training Institute (BRTI) in Harare, Zimbabwe, the Zimbabwean Ministries of Health and Childcare (MoHCC) and Primary and Secondary Education (MoPSE), the London School of Hygiene & Tropical Medicine (LSHTM) and the WHO, which has led to many collaborations, including research studies on young people’s health18,54, capacity strengthening (Southern Africa Research Capacity Network, https://www.sofarafrica.org/our-programme) and professional development55. Chitungwiza was selected by the BRTI as a study setting owing to its proximity to the research center in Harare and a long-established collaboration with Chitungwiza City Health. Formative work conducted in Chitungwiza in 2020 (ref. 18) and previous work with young people informed the study procedures and ethical considerations.
In keeping our focus on designing contextually relevant interventions, intervention and evaluation procedures were designed with Zimbabwean investigators and youth researchers, with regular input from an Adolescent Advisory Group from the study community and external expert advisors (national and international). Discussions with MoHCC and MoPSE and previous work from this region were used to guide the design of the study and have been taken into account in the citations for this paper. The study was coordinated by Zimbabwean researchers, and team members collaborated on data ownership, intellectual property and authorship of publications related to the work. Roles and responsibilities were agreed upon among researchers ahead of the research. The principal investigator (A.M.D.) and LSHTM researchers (V.S., R.A.F. and C.R.S.M.-Y.) were based full-time in Zimbabwe during the study implementation and provided technical support to the Zimbabwean study coordinator and to field and data teams. Two team members embedded their doctoral research within the Y-Check study. In addition, three master’s degrees, two bachelorʼs degrees and two diploma courses for Zimbabwean staff were supported within the Y-Check study.
Providers were specifically trained on how to communicate with and address the specific needs of LGBT+ clients. Where feasible, the needs of people with disabilities were addressed—for example, by providing support when completing questionnaires and adapting screening procedures. Standard operating procedures and training ensured that providers were safe—for example, post-exposure prophylaxis, safe lifting and handling procedures and keeping safe after hours. The study started toward the end of the COVID-19 pandemic, and personal protective equipment was provided to staff and participants, and staff were trained on infection prevention and control procedures.
Ethics approval
Ethics approval was granted by the institutional review boards of the Medical Research Council of Zimbabwe (MRCZ/A/2766), the institutional ethics committee of the Chitungwiza City Health Department, the LSHTM (26395) and the WHO (ERC.0003778). Primary school students aged 10–14 years and secondary school students aged 15–19 years could participate in the study if their parent/guardian consented and they also provided their assent. At community venues, adolescents aged 16–19 years provided their own informed consent. The study protocol and statistical analysis plan are available at https://doi.org/10.17037/DATA.00004763. The study is also registered at ClinicalTrials.gov: NCT06090006.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.