Dermatological manifestations of nutritional deficiencies often serve as the first clinical indicators of systemic health imbalances, ranging from vitamin and mineral shortages to protein-energy malnutrition. According to the National Institutes of Health (NIH) Office of Dietary Supplements, the skin—as the body’s largest organ—frequently reflects internal metabolic status through changes in texture, pigmentation, and hair or nail integrity. Recognizing these specific cutaneous markers allows clinicians to identify underlying dietary inadequacies before they progress to more severe systemic complications.
As a physician practicing in Berlin, I frequently observe how these signs are often overlooked in routine physical examinations. While many skin conditions are primary dermatological issues, a subset of patients presents with signs that are directly linked to micronutrient status. Understanding the difference between secondary dermatological symptoms of systemic disease and primary nutritional deficiencies is essential for accurate diagnosis and patient management.
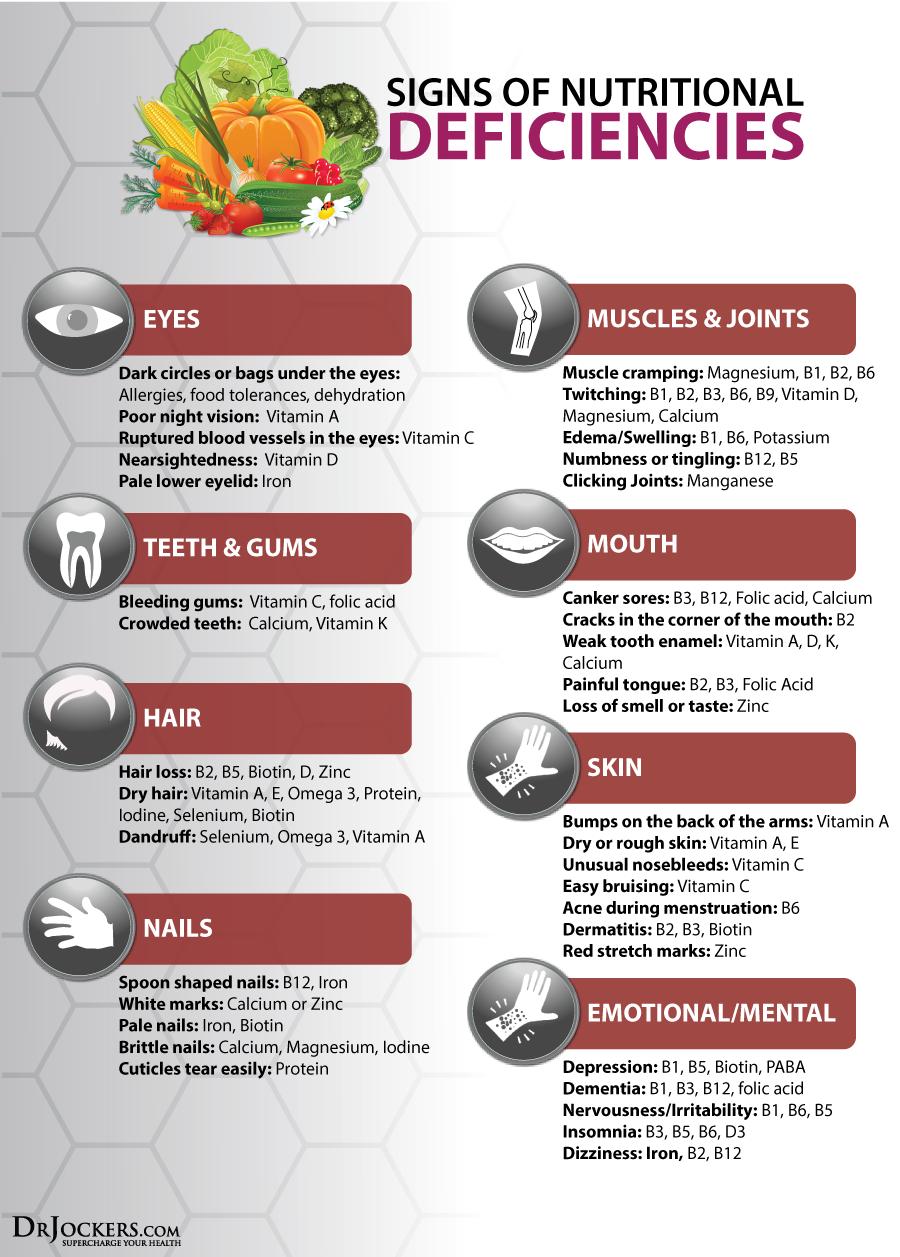
Identifying Skin Changes Linked to Vitamin Deficiencies
Specific vitamins play critical roles in skin barrier function, collagen synthesis, and cell turnover. When these essential nutrients are lacking, the skin often becomes the site of early clinical manifestation. For instance, vitamin C deficiency, while rare in developed nations, remains a recognized cause of perifollicular hemorrhage and corkscrew hairs, as documented by the National Center for Biotechnology Information (NCBI).

Vitamin A deficiency, or hypovitaminosis A, is widely associated with phrynoderma, commonly known as “toad skin.” This condition presents as follicular hyperkeratosis, where keratin plugs develop in the hair follicles, creating a rough, sandpapery texture, particularly on the extensor surfaces of the limbs. Furthermore, deficiencies in the B-vitamin complex, particularly niacin (B3), can lead to pellagra. According to the World Health Organization (WHO), the classic triad of pellagra includes dermatitis, diarrhea, and dementia, with the dermatitis often appearing as a symmetrical, photosensitive rash on sun-exposed areas.
Mineral Imbalances and Cutaneous Health
Minerals such as zinc and iron are vital for cellular proliferation and immune defense. Zinc deficiency, in particular, has a well-characterized dermatological profile. Acrodermatitis enteropathica, a condition resulting from severe zinc deficiency, presents with periorificial and acral dermatitis—rashes occurring around the mouth, anus, and on the extremities. The American Academy of Dermatology (AAD) notes that such rashes are often erythematous and scaly, and if left untreated, they can lead to secondary infections and hair loss, or alopecia.
Iron deficiency, while more commonly associated with anemia, also impacts the integumentary system. Individuals with chronic iron deficiency may exhibit koilonychia, or “spoon nails,” where the nail plate becomes concave and brittle. Pallor of the skin and mucous membranes is another standard clinical indicator, though it is often more reliably assessed in the conjunctiva than in the skin alone. These signs highlight the necessity of a comprehensive blood panel when dermatological symptoms appear alongside signs of general fatigue or malaise.
The Role of Protein and Essential Fatty Acids
Protein-energy malnutrition remains a primary concern globally, affecting skin integrity through the depletion of structural proteins. Kwashiorkor, a form of severe protein malnutrition, is characterized by “flaky paint” dermatosis, where the skin becomes hyperpigmented and peels in patches. This clinical sign is a direct result of the body’s inability to synthesize the proteins required for skin repair and pigment regulation, as outlined in clinical guidelines provided by the Centers for Disease Control and Prevention (CDC).
Essential fatty acid (EFA) deficiency is another factor that can compromise skin barrier function. Linoleic acid deficiency typically presents as dry, scaly skin and an inability to retain moisture, leading to increased transepidermal water loss. While rare in healthy populations, EFA deficiency can occur in patients with malabsorption syndromes or those on strictly controlled parenteral nutrition. In these cases, dermatological health is often restored once the lipid imbalance is corrected through targeted supplementation.
Diagnostic Approach and Clinical Management
When a patient presents with skin abnormalities that suggest a nutritional cause, a systematic diagnostic approach is required. Clinicians should first obtain a detailed dietary history, which may reveal restricted eating patterns, malabsorption issues such as celiac disease or inflammatory bowel disease, or reliance on processed foods. According to recent clinical reviews published in the Lancet, laboratory testing remains the gold standard for confirming suspected deficiencies, as physical signs alone are rarely pathognomonic.

Management involves addressing the root cause. Supplementation is often necessary to correct acute deficiencies, but the long-term solution lies in a balanced diet rich in whole foods. For patients with malabsorption, managing the underlying gastrointestinal pathology is just as critical as the nutritional replacement therapy itself. It is important to avoid self-supplementation, as excessive intake of certain vitamins—particularly fat-soluble vitamins like A and D—can lead to toxicity and further dermatological complications.
As medical research continues to evolve, our understanding of the skin’s role as a diagnostic window into nutritional status will likely expand. Future updates from international health authorities will continue to refine the criteria for identifying these deficiencies. Readers are encouraged to consult with their primary care physician before starting any new vitamin or mineral regimen. For those interested in public health updates, the European Food Safety Authority (EFSA) provides ongoing reports on dietary reference values and safety guidelines for the general population.
If you found this overview helpful, please share it with your community or leave a comment below. We welcome your questions on how diet impacts skin health, and we will address common queries in our next scheduled clinical review update.
Keep reading
- Since the provided text is only a small snippet of a larger story (mentioning Doctor Bustillo and Doctor Pedro over a span of four decades), it lacks the specific subject matter needed for a high-ranking SEO title. However, based on the context of medical legacy, nostalgia, and long-term professional relationships, here are the best options depending on the actual goal of the article: Option 1: Story-driven/Emotional (Best for Blogs/Memoirs) The Lasting Impact of Mentorship: Remembering Doctor Bustillo and Doctor Pedro Option 2: Professional/Biographical (Best for Institutional sites) Four Decades of Excellence: The Legacy of Doctor Bustillo and Doctor Pedro Option 3: SEO-Optimized/Broad (Best for Search Traffic) Medical Legacies: Honoring the Influence of Dr. Bustillo and Dr. Pedro If you provide the full article or the main topic (e.g., is it a tribute, a history of a clinic, or a personal memoir?), I can give you a 100% precise “perfect” title.
- Oxford University Begins Human Trials for ChAdOx1 Ebola Vaccine