
For decades, the medical community has faced a heartbreaking limitation in the treatment of preterm pre-eclampsia: the only definitive “cure” is the delivery of the baby. When this condition strikes early in a pregnancy, clinicians are often forced into a perilous balancing act, weighing the risk of maternal organ failure against the risks of extreme prematurity for the infant.
However, a recent first-in-human trial has introduced a potential paradigm shift. New research indicates that the selective removal of a specific placental protein, known as sFlt-1, is safe in humans. This development could mark the beginning of a new era of targeted therapy, offering a way to manage the disease’s underlying cause rather than simply managing its symptoms until delivery becomes inevitable.
As a physician and journalist, I have followed the evolution of maternal-fetal medicine closely. The move toward molecularly targeted interventions—treating the protein responsible for the pathology rather than just the resulting high blood pressure—represents a sophisticated leap forward. For mothers facing a preterm diagnosis, this could mean more time in the womb for the baby and a safer recovery for the parent.
The Biological Trigger: Understanding sFlt-1
To understand why the selective removal of sFlt-1 is so significant, we must first look at what happens inside a placenta during pre-eclampsia. In a healthy pregnancy, the placenta produces pro-angiogenic factors—proteins that encourage the growth and maintenance of healthy blood vessels. These include Vascular Endothelial Growth Factor (VEGF) and Placental Growth Factor (PlGF).

In cases of pre-eclampsia, this balance is disrupted. The placenta begins to overproduce a protein called soluble fms-like tyrosine kinase-1, or sFlt-1. This protein acts as a “decoy receptor.” Instead of allowing VEGF and PlGF to bind to the blood vessel walls to keep them healthy, sFlt-1 intercepts and binds to them first, neutralizing their beneficial effects.
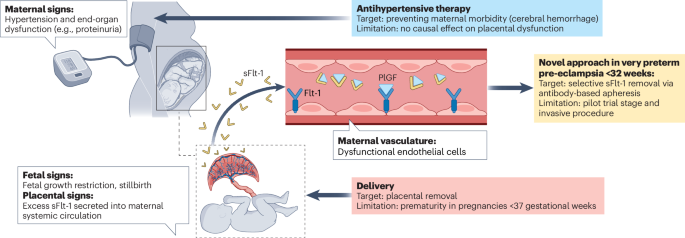
When these growth factors are neutralized, the mother’s blood vessels become dysfunctional. This leads to the hallmark signs of the condition: systemic hypertension (high blood pressure) and proteinuria (protein in the urine), which can escalate into seizures (eclampsia) or organ failure. Because pre-eclampsia can affect approximately millions of women globally, the need for a targeted intervention has been an urgent priority for public health.
Fig. 1: Clinical features and treatment options in pre-eclampsia.
A New Approach: Selective Protein Removal
Until now, treatment for preterm pre-eclampsia has largely focused on controlling blood pressure with antihypertensives and using corticosteroids to accelerate fetal lung development in anticipation of an early birth. The root cause—the excess of sFlt-1 circulating in the mother’s blood—remained untouched.
The recent first-in-human trial tested a method to selectively remove sFlt-1 from the maternal circulation. By targeting and extracting this specific protein, researchers aimed to restore the balance of pro-angiogenic factors, effectively “unblocking” the blood vessels and reducing the severity of the disease.
The primary goal of this initial trial was safety. In the world of clinical research, “first-in-human” studies are critical for establishing that a new intervention does not cause unforeseen harm. The results have provided critical safety data, confirming that the selective removal of sFlt-1 is feasible and well-tolerated. This clears the path for larger trials to determine exactly how much this treatment can extend a pregnancy and improve neonatal outcomes.
Why Targeted Therapy Changes the Game
The shift from general management to targeted therapy is a fundamental change in how we approach pregnancy complications. The implications are twofold: maternal stability and fetal maturity.
For the Mother: By reducing the levels of sFlt-1, clinicians may be able to mitigate the endothelial damage that leads to kidney dysfunction and liver stress. This reduces the immediate risk of life-threatening complications, potentially allowing for a more controlled and planned delivery.
For the Child: Every day a baby remains in the womb during the preterm window is critical. The difference between a birth at 28 weeks and 32 weeks is profound in terms of lung development, brain maturity, and overall survival rates. If targeted therapy can safely delay delivery by even a week or two, it could significantly reduce the incidence of neonatal intensive care unit (NICU) complications.
This approach moves us away from the “wait and see” model and toward a “treat and stabilize” model. Instead of treating the high blood pressure as the disease, we are treating the protein that causes the blood pressure to rise.
Challenges and the Road Ahead
While the safety data is a landmark achievement, several hurdles remain before this becomes a standard of care in hospitals worldwide. The process of selective removal—likely involving a form of apheresis or specialized filtration—is more complex than administering a pill or a standard IV drip. It requires specialized equipment and trained medical staff, which may limit its initial availability to tertiary care centers.

the medical community must determine the optimal timing for the intervention. Identifying the exact moment when sFlt-1 levels become pathological requires precise screening. The use of the sFlt-1/PlGF ratio is already becoming a tool for diagnosis in some regions, but integrating this into a treatment pipeline requires seamless coordination between diagnostic labs and clinical teams.
Future studies will need to focus on efficacy: Does removing sFlt-1 actually result in a statistically significant extension of pregnancy? Does it improve the long-term health of the mother? These are the questions that the next phase of clinical trials will answer.
Key Takeaways for Patients and Providers
- The Innovation: A new method allows for the selective removal of sFlt-1, a protein that triggers the symptoms of pre-eclampsia.
- Safety First: The first-in-human trial has successfully provided critical safety data, proving the procedure is viable.
- The Goal: To move beyond symptom management and provide a targeted therapy that could delay preterm birth.
- The Impact: Potential for improved maternal organ function and better fetal lung and brain development.
For those currently navigating a high-risk pregnancy, This proves important to remember that this treatment is in the early stages of clinical validation. It is not yet available as a general clinical option, but it provides a clear roadmap for the future of maternal health.
The next confirmed checkpoint for this research will be the transition to larger-scale efficacy trials, which will determine the impact of sFlt-1 removal on pregnancy duration and neonatal health outcomes. We expect further data as these trials progress through regulatory review.
Do you have questions about the latest innovations in maternal health? Share your thoughts in the comments below or share this article with a healthcare provider to start a conversation about the future of pre-eclampsia care.