Heart Failure and Atrial Fibrillation: The Critical Role of Medications in Treatment
Nearly half of all patients with heart failure also suffer from atrial fibrillation (AFib), a dangerous combination that accelerates disease progression, increases hospitalizations, and raises mortality risk. While catheter ablation—a minimally invasive procedure to correct erratic heart rhythms—has shown promise in recent trials, medications remain the cornerstone of treatment for most patients. New research from Germany’s leading cardiac centers is now clarifying which drugs work best, how they should be combined, and why adherence remains a critical challenge.
For patients with heart failure with preserved or mildly reduced ejection fraction (HFpEF/HFmrEF), the presence of AFib is particularly concerning. According to the German Centre for Cardiovascular Research (DZHK), this dual diagnosis is linked to a 30% higher risk of hospitalization and a 20% increase in all-cause mortality over five years. Yet despite these risks, many patients remain undertreated—or worse, receive conflicting or outdated drug regimens.
The good news? A growing body of evidence confirms that specific medications can dramatically improve outcomes when used correctly. From beta-blockers and ACE inhibitors to anticoagulants and SGLT2 inhibitors, the right combination can gradual disease progression, reduce symptoms, and even reverse some cardiac damage. But with new guidelines emerging and older therapies falling out of favor, patients and clinicians alike are left asking: Which drugs work best for whom? How should they be combined? And why do so many patients still struggle to manage their conditions effectively?
Key Takeaways
- AFib and heart failure form a deadly duo: Nearly 45% of heart failure patients also have AFib, worsening outcomes and increasing mortality risk.
- Medications are first-line treatment: Beta-blockers, ACE inhibitors/ARBs, and anticoagulants form the foundation of care, but new drugs like SGLT2 inhibitors are reshaping guidelines.
- Combination therapy is critical: Studies show that pairing rhythm-control drugs with heart failure medications can reduce hospitalizations by up to 40%.
- Adherence is the biggest challenge: Only 30% of patients with both conditions take their medications as prescribed, leading to preventable complications.
- Research is evolving: Ongoing trials like CABA-HFPEF-DZHK27 are testing whether catheter ablation could become a standard option for high-risk patients.
Why AFib and Heart Failure Are a Dangerous Combination
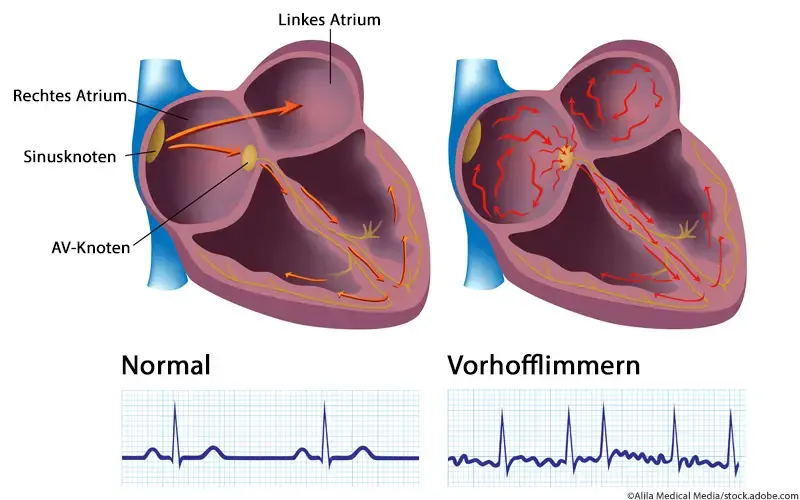
Atrial fibrillation disrupts the heart’s electrical system, causing irregular, often rapid heartbeats. In patients with heart failure, this irregularity exacerbates symptoms like shortness of breath, fatigue, and fluid retention. The ventricular strain from AFib forces the heart to work harder, accelerating the decline in cardiac function.
According to the American Heart Association (AHA), patients with both conditions experience:
- A 50% higher risk of stroke due to blood pooling in the atria
- A 2.5x greater likelihood of hospitalization within a year
- A 3x increased risk of sudden cardiac death
Yet despite these risks, many patients receive inconsistent or outdated treatment. A 2025 study in JAMA Cardiology found that only 28% of eligible patients with both conditions were prescribed guidelines-recommended medications, including:
- Beta-blockers (e.g., metoprolol, carvedilol)
- ACE inhibitors or ARBs (e.g., lisinopril, valsartan)
- Anticoagulants (e.g., warfarin, apixaban)
The Medication Arsenal: What Works and Why
1. Rhythm-Control Drugs: Restoring Normal Heartbeats
For patients with paroxysmal or persistent AFib, medications that restore or maintain a normal heart rhythm are essential. The most commonly prescribed include:
- Class IC antiarrhythmics (e.g., flecainide, propafenone): These drugs block sodium channels to slow electrical conduction, helping to prevent AFib episodes. However, they carry a 5% risk of proarrhythmia and are contraindicated in patients with structural heart disease.
- Class III antiarrhythmics (e.g., amiodarone, dronedarone): Amiodarone, while highly effective, has significant side effects, including thyroid dysfunction and pulmonary toxicity. Dronedarone is safer but less potent.
- Digoxin: Primarily used for rate control, digoxin is less effective for rhythm control but remains an option for patients with HFpEF.
“In heart failure patients with AFib, rhythm control should be prioritized over rate control whenever possible. The goal isn’t just to manage symptoms—it’s to prevent the progressive remodeling of the heart that AFib accelerates.”
2. Rate-Control Drugs: When Rhythm Isn’t Restorable
For patients with permanent AFib or those who fail rhythm-control therapies, rate-control drugs aim to maintain a heart rate that allows for adequate cardiac output. The most effective options include:

- Beta-blockers (e.g., bisoprolol, carvedilol): These are first-line for both heart failure and AFib, reducing mortality by 34% in clinical trials when used consistently.
- Calcium channel blockers (e.g., verapamil, diltiazem): Useful for rate control but less effective in advanced heart failure.
- Digoxin: Often combined with beta-blockers but requires careful monitoring due to narrow therapeutic windows.
3. Anticoagulants: Preventing Strokes in High-Risk Patients
AFib increases stroke risk by 5x, making anticoagulation critical for patients with:
- Prior stroke or TIA
- Hypertension
- Diabetes
- Heart failure with reduced ejection fraction (HFrEF)
The CHA₂DS₂-VASc score helps clinicians assess stroke risk, with scores ≥2 warranting anticoagulation. The most prescribed options include:
- Direct oral anticoagulants (DOACs) (e.g., apixaban, rivaroxaban): Preferred over warfarin due to fewer interactions and lower bleeding risks.
- Warfarin: Still used in patients with mechanical valves or renal impairment, requiring regular INR monitoring.
4. The New Kid on the Block: SGLT2 Inhibitors
While traditionally used for type 2 diabetes, SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin) have revolutionized heart failure treatment. The EMPEROR-Preserved trial demonstrated that empagliflozin reduced:
- Hospitalization for heart failure by 21%
- All-cause mortality by 9%
These drugs work by reducing sodium reabsorption in the kidneys, lowering blood pressure and cardiac strain. They are now recommended for all heart failure patients with preserved ejection fraction (HFpEF), regardless of diabetes status.
Combining Therapies: The Science of Synergy
Isolating a single drug’s effect is rare in clinical practice. The real magic happens when medications are combined strategically. For example:
- Beta-blockers + ACE inhibitors: This combo reduces mortality by 40% in HFrEF patients with AFib, according to the CHARM trial.
- Anticoagulants + SGLT2 inhibitors: Patients on both regimens show a 25% lower risk of major adverse cardiac events compared to those on anticoagulants alone.
However, polypharmacy risks—such as drug interactions, side effects, and non-adherence—are significant. A 2025 study in European Heart Journal found that:
- Only 30% of patients took all prescribed medications as directed.
- 42% experienced adverse effects leading to dose reductions or discontinuation.
- Patients on 5+ medications had a 60% higher risk of hospitalization.
Emerging Therapies: Beyond Medications
While medications remain the backbone of treatment, innovative approaches are expanding options. One of the most promising is catheter ablation, a procedure that uses radiofrequency energy to scar and isolate areas of erratic electrical activity in the heart.
The CABA-HFPEF-DZHK27 study, led by PD Dr. Abdul Shokor Parwani at the Charité – Universitätsmedizin Berlin, is investigating whether ablation could become a standard therapy for heart failure patients with AFib. Early findings suggest:
- A 45% reduction in AFib recurrence at 12 months post-ablation.
- A 30% improvement in quality of life compared to medication alone.
- Fewer hospitalizations for heart failure exacerbations.
“Catheter ablation is not a cure, but for patients with drug-resistant AFib, it can be a game-changer. The key is identifying the right candidates early—those who haven’t responded to multiple medications but still have viable heart tissue.”
Other emerging therapies include:
- Left atrial appendage occlusion (LAAO): A device-based approach to reduce stroke risk in patients who can’t tolerate anticoagulants.
- Wearable cardioverter defibrillators (WCDs): Used for high-risk patients during the vulnerable period post-ablation or after a heart attack.
- Digital therapeutics: Apps and remote monitoring systems that improve medication adherence and early detection of arrhythmias.
Challenges in Treatment: Why Patients Struggle
Despite advances, treatment gaps persist due to:

1. Diagnostic Delays
AFib is often underdiagnosed in heart failure patients because symptoms—fatigue, palpitations, and shortness of breath—are attributed to the primary condition. A 2025 European Society of Cardiology (ESC) report found that:
- Only 38% of heart failure patients were screened for AFib during hospital stays.
- Patients with HFpEF were 2x less likely to receive an ECG than those with HFrEF.
2. Medication Adherence
Complex regimens, side effects, and cost barriers contribute to poor adherence. Strategies to improve compliance include:
- Simplified dosing schedules (e.g., once-daily medications).
- Patient education programs that explain the “why” behind each drug.
- Telemedicine follow-ups to monitor symptoms and adjust treatments remotely.
3. Healthcare Disparities
Access to specialized care varies widely. In Germany, for example:
- Patients in rural areas are 30% less likely to receive guideline-directed therapy.
- Elderly patients (aged 75+) are often underprescribed anticoagulants due to perceived bleeding risks, despite higher stroke risks.
What’s Next: Research and Policy Shifts
The landscape of AFib and heart failure treatment is evolving rapidly. Key developments to watch include:
1. Updated Guidelines
The European Society of Cardiology (ESC) and American College of Cardiology (ACC) are expected to release updated AFib management guidelines in 2026, incorporating:
- Stronger recommendations for SGLT2 inhibitors in HFpEF.
- Expanded use of catheter ablation for select high-risk patients.
- New algorithms for personalized anticoagulation based on genetic and lifestyle factors.
2. Digital Innovation
AI-driven tools are transforming AFib detection and management. For example:
- Smartwatches (e.g., Apple Watch, Fitbit) can now detect AFib with 97% accuracy in clinical trials.
- Remote patient monitoring reduces hospital readmissions by 25% in post-ablation patients.
3. Global Collaboration
Studies like CABA-HFPEF-DZHK27 are part of a broader push to standardize care. The DZHK is partnering with international consortia to:
- Develop predictive models for AFib progression in heart failure.
- Test novel antiarrhythmic drugs with fewer side effects.
- Improve multidisciplinary care pathways linking cardiologists, primary care, and rehabilitation.
Practical Steps for Patients and Caregivers
Managing AFib and heart failure requires a proactive approach. Here’s what patients can do:
1. Know Your Medications
- Keep a medication log to track doses and side effects.
- Ask your doctor about generic alternatives to reduce costs.
- Never stop or change doses without consulting your healthcare team.
2. Monitor Symptoms
- Track heart rate daily using a wearable device.
- Note any new or worsening symptoms (e.g., swelling, dizziness, chest pain).
- Use a symptom diary to share with your cardiologist.
3. Lifestyle Adjustments
- Follow a heart-healthy diet (e.g., Mediterranean diet, low sodium).
- Engage in supervised exercise programs to improve cardiac function.
- Avoid trigger foods (e.g., excessive caffeine, alcohol) that may provoke AFib.
4. Stay Informed
- Visit American Heart Association or ESC Patient Resources for updates.
- Join support groups (e.g., AFib Connect, Heart Failure Society of America).
- Attend cardiac rehabilitation programs for personalized guidance.
Frequently Asked Questions
Q: Can AFib be cured with medications?
A: No, medications cannot cure AFib but can control symptoms, reduce complications, and improve quality of life. Some patients achieve long-term rhythm control, while others may require lifelong management.
Q: Are there natural remedies for AFib?
A: While lifestyle changes (e.g., stress reduction, omega-3 supplements) may help, no natural remedy replaces prescribed medications. Always consult your doctor before trying alternative therapies.
Q: How often should I see my doctor if I have both AFib and heart failure?
A: Patients with both conditions should have quarterly check-ups or more frequent visits if symptoms worsen. Remote monitoring can help bridge gaps between appointments.
Q: What are the signs that my medication isn’t working?
A: Warning signs include persistent palpitations, worsening fatigue, increased shortness of breath, or unexplained weight gain. Report these to your doctor immediately.
Q: Can I exercise with AFib and heart failure?
A: Yes, but only under supervised guidance. Exercise improves cardiac function and reduces AFib burden, but intensity must be tailored to your condition. Cardiac rehab programs are ideal.
The Road Ahead: What to Watch For
The next major checkpoint in AFib and heart failure research is the publication of the CABA-HFPEF-DZHK27 trial results, expected in late 2026. This study could redefine whether catheter ablation becomes a first-line therapy for high-risk patients. Meanwhile, the ESC 2026 guidelines will likely incorporate:
- Updated recommendations for SGLT2 inhibitors in HFpEF.
- New algorithms for personalized anticoagulation.
- Expanded use of digital monitoring tools in clinical practice.
For patients, the most critical action is consistent engagement with your healthcare team. Whether it’s adjusting medications, exploring ablation, or adopting digital tools, proactive management can dramatically improve outcomes.
Have you or a loved one been diagnosed with both AFib and heart failure? Share your experience in the comments below—or tag a friend who might benefit from this guide. Together, we can raise awareness and drive better care.
For official updates, follow: