Medical researchers are currently advancing allergen immunotherapy (AIT) to move beyond symptom management toward a long-term cure for allergies. While no single “miracle cure” exists for all patients, clinical evidence from the American Academy of Allergy, Asthma & Immunology shows that immunotherapy can modify the immune system’s response to specific triggers, potentially providing years of relief or permanent desensitization.
Allergies affect approximately 30% of the population in some regions, including France, where heatwaves often accelerate pollen release and trigger widespread respiratory distress. The current medical gold standard for those seeking more than temporary relief is immunotherapy, which involves exposing the patient to gradually increasing doses of an allergen to build tolerance. This process differs fundamentally from antihistamines, which only block the symptoms after an allergic reaction has already begun.
The search for a universal cure is complicated by the diversity of the human immune system and the variety of triggers, ranging from seasonal pollens to perennial dust mites and food proteins. However, the shift toward “precision medicine” is allowing doctors to tailor these treatments to a patient’s specific IgE antibody profile, increasing the success rate of desensitization protocols.
How Allergen Immunotherapy Works to Desensitize the Body
Allergen immunotherapy (AIT) aims to retrain the immune system to stop treating harmless substances, like ragweed or birch pollen, as dangerous threats. According to the World Allergy Organization, the goal is to shift the immune response from a Th2-mediated allergic reaction to a Th1-mediated tolerant response, often involving the production of IgG4 antibodies that block the allergic trigger before it can activate mast cells.
There are two primary delivery methods for this treatment. Subcutaneous immunotherapy (SCIT) involves injections administered in a clinical setting over several years. Oral immunotherapy (OIT), more common in food allergy treatments, involves ingesting tiny, measured amounts of the allergen. While SCIT is widely used for respiratory allergies, OIT is frequently employed for peanut and tree nut allergies to prevent life-threatening anaphylaxis.
The effectiveness of these treatments varies. Some patients achieve complete clinical tolerance, meaning they no longer react to the allergen even after stopping treatment. Others experience a significant reduction in symptoms that requires “maintenance” doses to sustain. The duration of the treatment typically ranges from three to five years to ensure the immune system’s “memory” is permanently altered.
The Impact of Climate Change on Pollen Levels and Allergy Prevalence
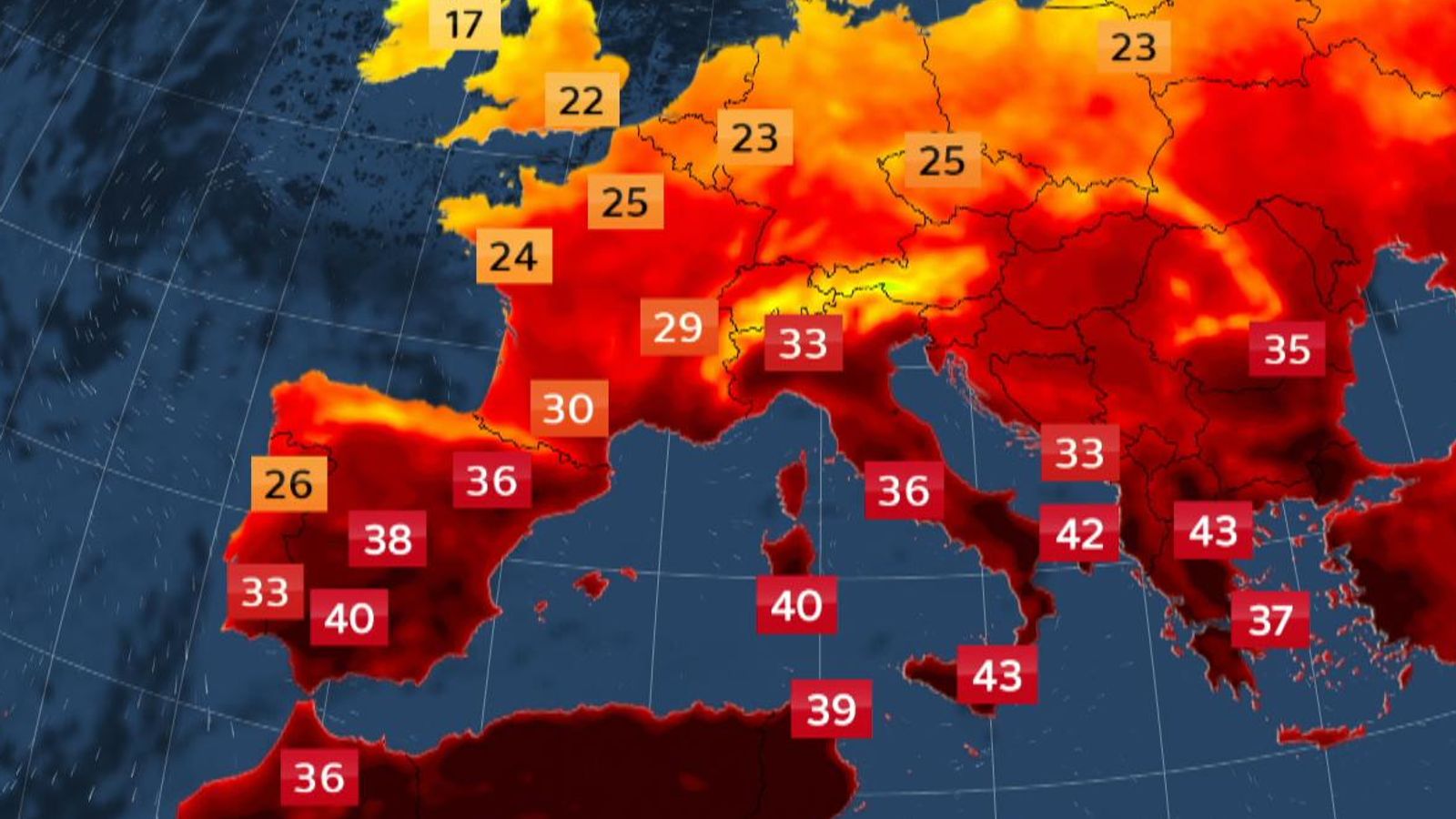
Environmental factors are making the management of allergies more difficult. Rising global temperatures and increased CO2 levels contribute to longer pollination seasons and higher pollen concentrations. In France, recent heatwaves have led to high-alert warnings across dozens of departments as pollen counts spike, affecting a significant portion of the population.

Higher temperatures do not just trigger the release of pollen; they can increase the potency of the pollen itself. Research indicates that plants grown in high-CO2 environments often produce more pollen proteins, which can make allergic reactions more severe. This environmental pressure increases the demand for long-term solutions like immunotherapy, as traditional medications may not be sufficient to counter the increased allergen load in the air.
For those suffering from seasonal allergic rhinitis, the timing of the “pollen peak” is critical. Medical professionals advise starting immunotherapy several months before the season begins—typically in autumn or winter—to ensure the body is desensitized before the first wave of spring pollens arrives.
Comparing Traditional Treatments vs. Long-Term Immunotherapy
To understand why immunotherapy is viewed as the closest thing to a “cure,” it is necessary to compare it with standard pharmacological interventions.
| Treatment Type | Mechanism | Duration of Effect | Primary Goal |
|---|---|---|---|
| Antihistamines | Blocks H1 receptors to stop histamine action | Hours to Days | Symptom relief |
| Corticosteroids | Reduces inflammation in nasal passages | Days to Weeks | Inflammation control |
| Immunotherapy (AIT) | Modifies immune system tolerance | Years or Permanent | Disease modification |
While antihistamines are essential for immediate comfort, they do not change the underlying cause of the allergy. According to clinical guidelines, AIT is the only treatment capable of altering the natural course of the disease and potentially preventing the development of asthma in patients who only have allergic rhinitis.
The Future of Allergy Cures: Biologics and Gene Therapy
Beyond traditional AIT, the medical community is exploring biologics—engineered proteins that target specific parts of the immune cascade. Monoclonal antibodies, such as Omalizumab, target IgE antibodies to prevent them from binding to mast cells. While these are not “cures” in the sense that they require ongoing administration, they provide a level of control for severe, treatment-resistant allergies that was previously impossible.
Research into “inverse vaccines” is also underway. Unlike traditional vaccines that teach the immune system to attack a pathogen, inverse vaccines aim to teach the immune system to ignore a specific protein. By targeting the dendritic cells in the liver or lungs, researchers hope to induce a state of systemic tolerance without the need for years of repeated injections.
The integration of genomic sequencing is also allowing physicians to identify why some people respond to immunotherapy while others do not. By analyzing the HLA (Human Leukocyte Antigen) genes, doctors may soon be able to predict with high accuracy whether a specific patient will achieve a permanent cure through AIT or if they should move directly to biologic therapies.
Practical Guidance for Allergy Sufferers
For individuals looking to move beyond daily medication, the first step is a comprehensive allergy panel to identify the exact proteins causing the reaction. This typically involves skin prick tests or RAST (Radioallergometric Extract Testing) blood tests.

Patients considering immunotherapy should be aware of the risks, most notably the possibility of a systemic allergic reaction (anaphylaxis) during the initial dosing phase. This is why SCIT must be performed in a medical facility equipped with epinephrine. Those pursuing OIT must follow strict dosing schedules and keep rescue medication on hand at all times.
Official health advisories recommend monitoring local pollen counts through government environmental agencies to time medication and outdoor activities. In Europe, the European Allergy and Clinical Immunology Organization (EAACI) provides updated guidelines on the management of allergic diseases to help patients navigate these options.
The next major milestone in allergy research involves the conclusion of several large-scale Phase III clinical trials for oral desensitization tablets, which aim to replace injections with a more convenient home-based regimen. Further updates on these trials are expected in upcoming medical congresses throughout 2025.
Do you have experience with immunotherapy, or are you considering it as an alternative to daily medication? Share your thoughts and questions in the comments below.