New Dyslipidemia Guidelines: A Practical Guide for Community Pharmacists
Berlin, Germany — In a significant update to cardiovascular care, the American College of Cardiology (ACC) and the American Heart Association (AHA) have released new clinical guidelines for the management of dyslipidemia, a condition characterized by abnormal lipid levels in the blood. These guidelines, published in late 2025, emphasize a more personalized approach to cholesterol management, integrating the latest evidence on lipid-lowering therapies and their real-world application. For community pharmacists—often the most accessible healthcare providers for patients—these updates present both opportunities and challenges in ensuring safe and effective medication use.
Dyslipidemia is a major risk factor for atherosclerotic cardiovascular disease (ASCVD), which remains the leading cause of death worldwide. With an estimated 28% of adults globally affected by elevated low-density lipoprotein cholesterol (LDL-C), the role of pharmacists in managing this condition has never been more critical. The new ACC/AHA guidelines introduce key changes, including updated risk assessment tools, expanded indications for non-statin therapies, and a stronger focus on patient-centered care. But how can community pharmacists translate these recommendations into everyday practice?
Dr. Helena Fischer, Editor of Health at World Today Journal and a physician with over a decade of experience in internal medicine, explores the practical implications of these guidelines for pharmacists on the front lines of patient care.
Key Changes in the 2025 ACC/AHA Dyslipidemia Guidelines
The 2025 ACC/AHA guidelines build on previous iterations but introduce several notable updates. One of the most significant shifts is the expansion of risk assessment tools to include social determinants of health, such as socioeconomic status, access to care, and environmental factors. This reflects a growing recognition that cardiovascular risk is influenced by more than just lipid levels and traditional risk factors like hypertension or diabetes. For pharmacists, this means considering a patient’s broader context when counseling on medication adherence or lifestyle modifications.
Another major update is the inclusion of newer non-statin therapies, such as PCSK9 inhibitors and bempedoic acid, as first-line options for certain high-risk patients. These drugs, while highly effective, come with higher costs and complex administration requirements, posing challenges for pharmacists in both counseling and access. The guidelines also emphasize the importance of shared decision-making, encouraging pharmacists to engage patients in conversations about their treatment goals and preferences.
Perhaps most relevant to community pharmacists is the updated guidance on drug-drug interactions, particularly with statins like atorvastatin. Statins remain the cornerstone of dyslipidemia management, but their interactions with other medications—such as antifungals, antibiotics, and certain heart medications—can lead to adverse effects, including muscle toxicity and liver dysfunction. The new guidelines provide clearer recommendations for monitoring and managing these interactions, which is especially important in community settings where patients may be taking multiple medications.
Why Community Pharmacists Are on the Front Lines
Community pharmacists are uniquely positioned to implement these guidelines. Unlike physicians, who may see patients only a few times a year, pharmacists interact with patients frequently—often monthly—when they pick up prescriptions or seek advice on over-the-counter medications. This regular contact allows pharmacists to monitor adherence, identify potential drug interactions, and provide ongoing education about lifestyle changes and medication management.
A recent nationwide study in Egypt highlighted the critical role of community pharmacists in managing atorvastatin-related drug interactions. The study found that while pharmacists were generally aware of common interactions, gaps remained in their ability to counsel patients effectively, particularly in busy or under-resourced settings. This underscores the need for targeted training and resources to support pharmacists apply the new guidelines in their daily practice.
For example, pharmacists can play a key role in identifying patients who may benefit from non-statin therapies but are hesitant due to cost or side effects. By discussing the risks and benefits of these medications—and exploring options like patient assistance programs—pharmacists can help bridge the gap between clinical recommendations and real-world access. They can also educate patients on the importance of regular lipid monitoring and lifestyle modifications, such as diet and exercise, which are cornerstones of dyslipidemia management.
Practical Steps for Implementing the Guidelines
So, how can community pharmacists position these guidelines into action? Here are some practical steps:
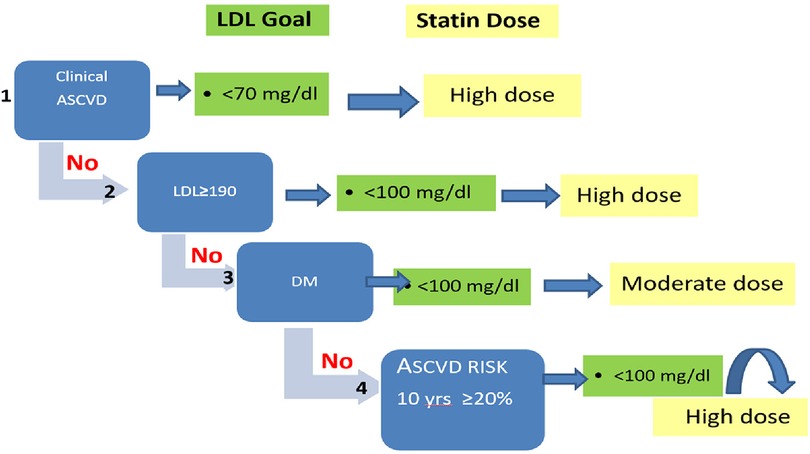
- Stay Updated on Risk Assessment Tools: The new guidelines recommend using tools like the ASCVD Risk Estimator Plus to evaluate a patient’s 10-year risk of cardiovascular events. Pharmacists can familiarize themselves with these tools and use them to guide conversations with patients about their risk factors and treatment options.
- Monitor for Drug Interactions: Pharmacists should review patients’ medication lists for potential interactions with statins and other lipid-lowering drugs. For example, atorvastatin can interact with medications like clarithromycin, fluconazole, and cyclosporine, increasing the risk of muscle toxicity. The guidelines recommend adjusting doses or switching to alternative therapies when interactions are identified.
- Educate Patients on Adherence: Non-adherence to lipid-lowering therapies is a major barrier to effective dyslipidemia management. Pharmacists can use tools like medication synchronization programs, which align refill dates for multiple prescriptions, to improve adherence. They can also provide clear, jargon-free explanations of why these medications are important and how to manage side effects.
- Advocate for Access to Non-Statin Therapies: For patients who cannot tolerate statins or need additional lipid-lowering effects, pharmacists can advocate for access to non-statin therapies. This may involve working with prescribers to explore alternatives, such as PCSK9 inhibitors or ezetimibe, and helping patients navigate insurance coverage or patient assistance programs.
- Promote Lifestyle Modifications: While medications are a critical component of dyslipidemia management, lifestyle changes—such as a heart-healthy diet, regular exercise, and smoking cessation—can significantly improve outcomes. Pharmacists can provide resources and referrals to support these changes, such as local nutrition programs or smoking cessation clinics.
Challenges and Opportunities
Despite their critical role, community pharmacists face several challenges in implementing the new guidelines. One of the biggest hurdles is time constraints. In many community pharmacies, pharmacists are responsible for dispensing medications, counseling patients, and managing administrative tasks, leaving little time for in-depth conversations about lipid management. The guidelines emphasize the importance of shared decision-making, but this requires time and resources that may not always be available.
Another challenge is the cost of newer lipid-lowering therapies. While drugs like PCSK9 inhibitors are highly effective, their high price can be a barrier for many patients. Pharmacists can help by identifying cost-saving strategies, such as generic alternatives or patient assistance programs, but these solutions are not always straightforward. Navigating insurance coverage for these medications can be complex, requiring pharmacists to stay up-to-date on formulary changes and prior authorization requirements.
Although, these challenges also present opportunities for pharmacists to demonstrate their value as integral members of the healthcare team. By taking a proactive role in dyslipidemia management, pharmacists can improve patient outcomes, reduce healthcare costs, and strengthen their relationships with both patients and prescribers. For example, pharmacists can collaborate with physicians to develop care plans that align with the new guidelines, ensuring that patients receive the most appropriate and effective treatments.
Key Takeaways for Pharmacists
To help community pharmacists navigate the new guidelines, here are some key takeaways:
- Personalized Risk Assessment: Use tools like the ASCVD Risk Estimator Plus to evaluate patients’ cardiovascular risk and tailor treatment recommendations accordingly.
- Drug Interaction Monitoring: Be vigilant about potential interactions with statins and other lipid-lowering therapies, and adjust treatment plans as needed.
- Patient Education: Provide clear, concise information about the importance of medication adherence and lifestyle modifications, and address any concerns or misconceptions patients may have.
- Access to Non-Statin Therapies: Advocate for patients who may benefit from newer lipid-lowering drugs, and help them navigate insurance coverage and cost barriers.
- Collaboration with Prescribers: Work closely with physicians to develop care plans that align with the new guidelines and ensure continuity of care.
Looking Ahead
The release of the 2025 ACC/AHA dyslipidemia guidelines marks a significant step forward in cardiovascular care. For community pharmacists, these updates provide a roadmap for improving patient outcomes through personalized, evidence-based care. However, implementing these guidelines will require ongoing education, collaboration, and advocacy to overcome the challenges of time constraints, cost barriers, and complex medication regimens.
As the healthcare landscape continues to evolve, the role of pharmacists in managing chronic conditions like dyslipidemia will only grow in importance. By staying informed, engaging with patients, and working closely with other healthcare providers, pharmacists can help ensure that the promise of these new guidelines translates into better health for millions of people worldwide.
The next official update from the ACC and AHA is expected in early 2027, with potential refinements to the guidelines based on emerging evidence. In the meantime, pharmacists are encouraged to review the full guidelines and explore resources like the ACC’s lipid management toolkit to support their practice.
Have you encountered challenges in implementing the new dyslipidemia guidelines in your pharmacy? Share your experiences in the comments below, and don’t forget to share this article with colleagues who may discover it helpful.