Managing Parkinson’s disease is often described by neurologists as a delicate balancing act. For millions of people worldwide, the introduction of dopaminergic medications brings a transformative return of mobility, a reduction in tremors, and a renewed sense of independence. However, this relief often comes with a complex set of trade-offs. As the disease progresses, the very drugs used to treat the symptoms can trigger serious side effects that may, in some cases, become as debilitating as the condition itself.
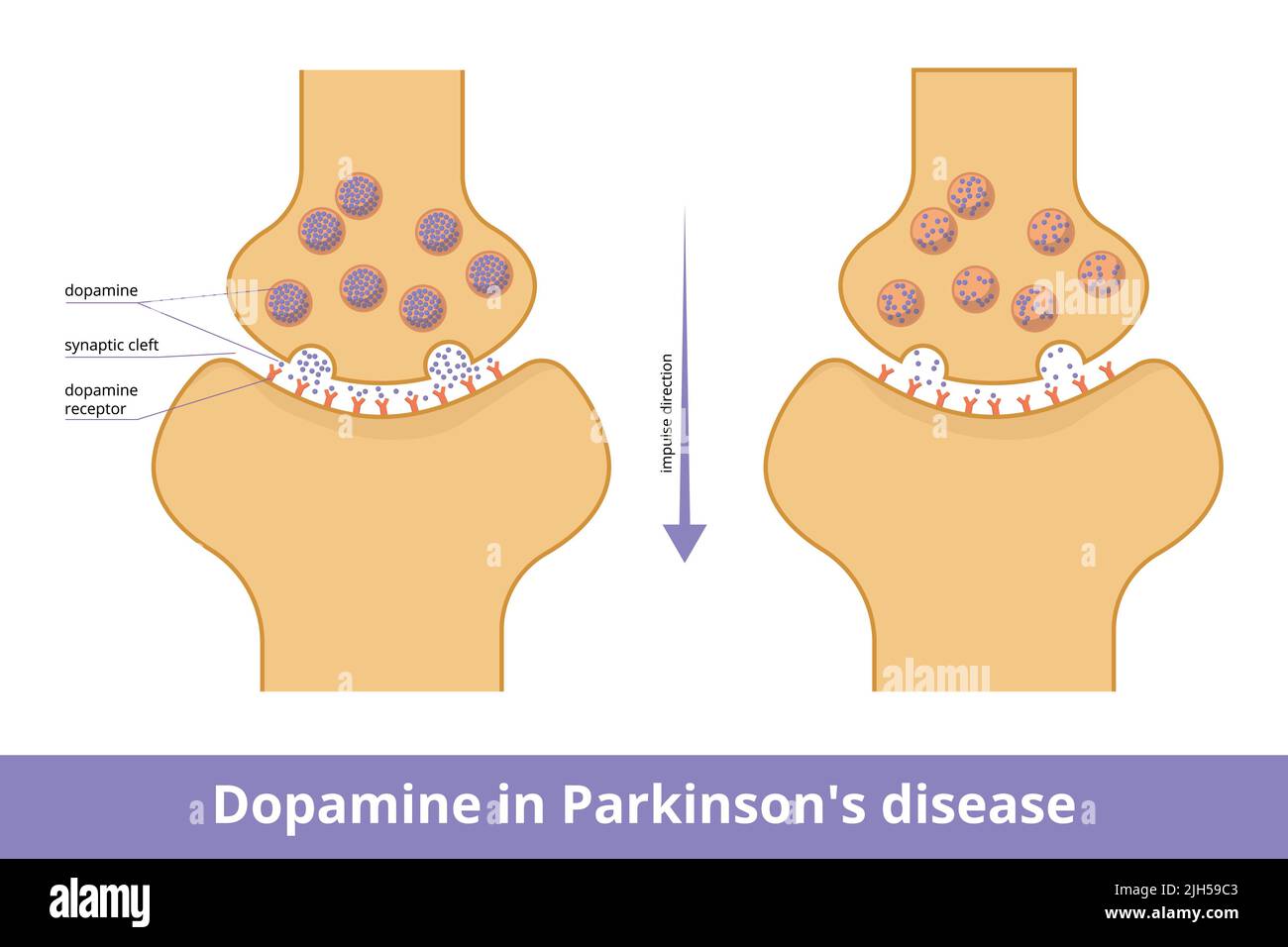
The central challenge lies in the brain’s chemistry. Parkinson’s is a progressive neurodegenerative disorder characterized by the loss of neurons in the substantia nigra, a region of the brain responsible for producing dopamine. Dopamine acts as a chemical messenger that allows for smooth, coordinated muscle movement. When these neurons die, the resulting dopamine deficiency leads to the hallmark symptoms of the disease: rigidity, bradykinesia (slowness of movement), and resting tremors.
While modern pharmacology can replenish these dopamine levels or mimic the neurotransmitter’s effects, the brain does not always respond linearly to these interventions. Over time, the window between a dose that is “too low” (leaving the patient immobile) and “too high” (triggering involuntary movements or psychiatric issues) narrows. Understanding these Parkinson’s disease medication side effects is critical for patients, caregivers, and healthcare providers to ensure that quality of life is maintained throughout the treatment journey.
As a physician and health journalist, I have seen how the psychological burden of these side effects can be overlooked in favor of motor improvements. It is not enough to simply “stop the shake”; we must ensure that the treatment does not inadvertently compromise a patient’s mental health, behavioral stability, or cognitive function. Navigating this terrain requires a proactive partnership between the patient and their neurology team, characterized by rigorous monitoring and a willingness to adjust therapies as the disease evolves.
The Gold Standard and Its Complications: Levodopa
For decades, Levodopa has remained the most effective treatment for the motor symptoms of Parkinson’s. Because dopamine cannot cross the blood-brain barrier, Levodopa serves as a precursor that the brain converts into dopamine. Often paired with carbidopa to prevent the drug from breaking down before it reaches the brain, this combination therapy significantly improves muscle control and coordination.
However, long-term use of Levodopa is frequently associated with a phenomenon known as Levodopa-induced dyskinesia (LID). Dyskinesia manifests as involuntary, erratic, dance-like movements of the arms, legs, or trunk. These movements are not a symptom of Parkinson’s itself, but rather a side effect of the medication. According to the Parkinson’s Foundation, these involuntary movements often occur when the medication is at its peak concentration in the bloodstream, creating a paradoxical situation where the drug designed to stop tremors creates a different form of uncontrolled movement.

Another significant challenge is the “wearing-off” effect. In the early stages of treatment, a single dose may provide relief for several hours. As the disease progresses and the brain loses more of its ability to store dopamine, the medication’s effectiveness lasts for shorter periods. This leads to “off” episodes, where symptoms return abruptly before the next dose is due. This fluctuation can cause intense anxiety and physical distress, often prompting patients to request higher doses, which in turn increases the risk of dyskinesia.
Dopamine Agonists and the Risk of Impulse Control Disorders
To delay the start of Levodopa or to reduce its dosage, doctors often prescribe dopamine agonists. Unlike Levodopa, which the brain converts to dopamine, agonists mimic dopamine by stimulating the dopamine receptors directly. While effective for many, these medications carry a specific and often devastating risk: Impulse Control Disorders (ICDs).
ICDs are behavioral side effects that can radically alter a patient’s personality and life. These include compulsive gambling, hypersexuality, binge eating, and compulsive shopping. These behaviors are not caused by the disease’s cognitive decline, but are a direct pharmacological response to the overstimulation of the brain’s reward system. The National Institute of Neurological Disorders and Stroke (NINDS) notes that these medications can trigger a “reward-seeking” loop in the brain, leading patients to engage in risky behaviors they would have previously avoided.
The danger of ICDs is that they are often invisible to the physician during a standard motor-function exam. A patient may appear physically stable and “well-controlled” while simultaneously experiencing a financial or familial crisis due to compulsive behaviors. This underscores the necessity of involving caregivers in the clinical conversation, as family members are typically the first to notice these behavioral shifts.
Psychiatric and Autonomic Side Effects
Beyond motor and behavioral changes, dopaminergic therapies can impact the mind and the body’s automatic functions. Hallucinations and delusions are relatively common, particularly in older adults or those with pre-existing cognitive impairment. These can range from mild visual distortions (seeing things that aren’t there) to full-blown psychotic episodes. When hallucinations occur, it often signals that the dopamine levels in certain parts of the brain have become too high, necessitating a careful titration of medication.
many Parkinson’s medications can cause orthostatic hypotension—a sudden drop in blood pressure upon standing. This can lead to dizziness, fainting, and a significantly increased risk of falls. For a population already struggling with balance and gait, a sudden drop in blood pressure can be catastrophic, leading to fractures or head injuries.
Nausea and gastrointestinal distress are also frequent early-stage side effects. While these are generally less “serious” than impulse control disorders, they can lead to medication non-compliance, which allows Parkinson’s symptoms to flare up, creating a cycle of instability that is hard to break.
Strategies for Mitigation and Management
The goal of Parkinson’s treatment is not the total elimination of symptoms—which is currently impossible—but the optimization of function with the minimum necessary medication. When serious side effects emerge, several clinical strategies can be employed:
- Dose Fractionation: Instead of fewer large doses, doctors may prescribe smaller, more frequent doses to smooth out the “peaks and valleys” of medication levels, reducing both “off” periods and dyskinesia.
- Medication Rotation: Switching from a dopamine agonist to a different class of drug, such as an MAO-B inhibitor, may reduce the risk of impulse control disorders while still providing symptomatic relief.
- Adjunctive Therapies: The use of Amantadine can sometimes help reduce the severity of Levodopa-induced dyskinesia.
- Surgical Intervention: For patients with severe motor fluctuations or refractory dyskinesia, Deep Brain Stimulation (DBS) may be an option. By delivering electrical impulses to specific brain regions, DBS can often reduce the need for high doses of medication, thereby mitigating the associated side effects.
Summary of Medication Risks and Effects
| Medication Class | Primary Goal | Serious Side Effects to Monitor |
|---|---|---|
| Levodopa/Carbidopa | Dopamine replacement | Dyskinesia, “wearing-off” effect, nausea |
| Dopamine Agonists | Mimic dopamine | Impulse control disorders, sudden sleep onset, edema |
| MAO-B Inhibitors | Prevent dopamine breakdown | Insomnia, orthostatic hypotension, interactions with other drugs |
| Anticholinergics | Reduce tremors | Confusion, blurred vision, urinary retention, memory loss |
Practical Guidance for Patients and Caregivers
Because the side effects of Parkinson’s medications can be subtle or embarrassing, patients often hesitate to report them. However, early detection is the only way to prevent permanent life disruptions, such as financial ruin from gambling or severe falls from hypotension.
What to track: Caregivers should keep a “symptom diary” that records not just the tremors and rigidity, but also mood swings, unusual spending habits, and the exact timing of when medications are taken versus when side effects appear. This data is invaluable for a neurologist when adjusting dosages.
When to call the doctor immediately:
- The onset of vivid hallucinations or delusions.
- New, compulsive behaviors (e.g., sudden obsession with gambling or shopping).
- Severe dizziness or fainting upon standing.
- Involuntary movements that interfere with eating, walking, or sleeping.
It is also essential to review all medications with a pharmacist. Some common over-the-counter drugs or medications for other conditions (such as certain antidepressants or blood pressure meds) can interact with Parkinson’s therapies, either neutralizing their effect or exacerbating the side effects.
The Path Forward: Beyond Symptom Management
The current pharmacological approach to Parkinson’s is primarily symptomatic; it treats the effects of dopamine loss without stopping the loss of the neurons themselves. The “holy grail” of Parkinson’s research is the development of disease-modifying therapies—treatments that can gradual, stop, or reverse the neurodegenerative process.
Current research is exploring several promising avenues, including monoclonal antibodies designed to clear alpha-synuclein (the protein that clumps in Parkinson’s brains) and stem cell therapies aimed at replacing the lost dopaminergic neurons in the substantia nigra. If these therapies prove successful, the reliance on high-dose dopaminergic drugs—and the accompanying risk of serious side effects—could be significantly reduced.
Until then, the priority remains a personalized, vigilant approach to care. The “best” medication is not the one that provides the most movement, but the one that provides the best overall quality of life, balancing physical mobility with mental and behavioral stability.
The next major milestone for the community will be the results of ongoing Phase III clinical trials for several new alpha-synuclein targeting therapies, which may provide the first real evidence of a disease-modifying treatment. We will continue to monitor these developments as they move toward regulatory review.
Do you or a loved one manage Parkinson’s disease? Which aspects of medication management have been the most challenging? Share your experiences in the comments below to help others in the community feel less alone in this journey.