Understanding Premenstrual Dysphoric Disorder: Why PMDD is More Than Just Severe PMS
Premenstrual Dysphoric Disorder (PMDD) is a severe, clinically recognized medical condition characterized by intense emotional and physical symptoms that significantly impair daily functioning. While many people experience premenstrual syndrome (PMS), PMDD is a distinct mental health disorder that often requires specialized medical intervention and can take years to correctly diagnose.
For many patients, the journey to a correct diagnosis is characterized by years of medical uncertainty and misunderstood symptoms. This struggle has fueled growing global awareness campaigns, including endurance-based efforts like long-distance walks, intended to bring visibility to the debilitating nature of the condition and the need for better clinical recognition.
Medical professionals distinguish PMDD from standard PMS based on the severity of psychological symptoms and the degree of functional impairment. According to the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5), PMDD is categorized as a depressive disorder characterized by significant mood disturbances during the luteal phase of the menstrual cycle.
How can you tell the difference between PMS and PMDD?
The primary distinction between premenstrual syndrome (PMS) and PMDD lies in the intensity of the emotional symptoms and their ability to disrupt a person’s ability to work, maintain relationships, or manage daily responsibilities. While PMS involves manageable discomforts, PMDD can lead to profound psychological distress.
Clinical observations suggest that while physical symptoms like bloating or breast tenderness may overlap, the psychological “overdrive” seen in PMDD is the defining factor. Those suffering from PMDD often experience extreme irritability, sudden outbursts of anger, or intense feelings of hopelessness that feel disconnected from their baseline personality.
| Feature | Premenstrual Syndrome (PMS) | Premenstrual Dysphoric Disorder (PMDD) |
|---|---|---|
| Primary Focus | Physical discomfort and mild mood shifts. | Severe emotional and psychological distress. |
| Emotional Severity | Mild irritability or sadness. | Intense anxiety, depression, or rage. |
| Daily Impact | Annoyance or slight disruption to routine. | Significant impairment in social or work life. |
| Clinical Status | Common symptomatic cluster. | Formal medical/psychiatric diagnosis. |
Why is PMDD often misdiagnosed for years?
The difficulty in securing a PMDD diagnosis often stems from the cyclical nature of the disorder. Because symptoms appear and disappear in alignment with the menstrual cycle, patients may only present to doctors when they are in their follicular phase—the period after menstruation when they feel healthy. This leads clinicians to overlook the hormonal connection.
Medical experts note that the lack of consistent symptom reporting during clinical visits frequently results in PMDD being misdiagnosed as general depression, anxiety disorders, or bipolar disorder. Without a detailed, multi-month tracking of symptoms, the cyclical pattern remains invisible to healthcare providers.
To achieve a formal diagnosis, the DSM-5 requires that symptoms occur in the week before the onset of menstruation and improve within a few days after menses begins. This requires patients to maintain rigorous daily symptom logs, a process that can be difficult to sustain without provider guidance.
What are the primary symptoms of PMDD?
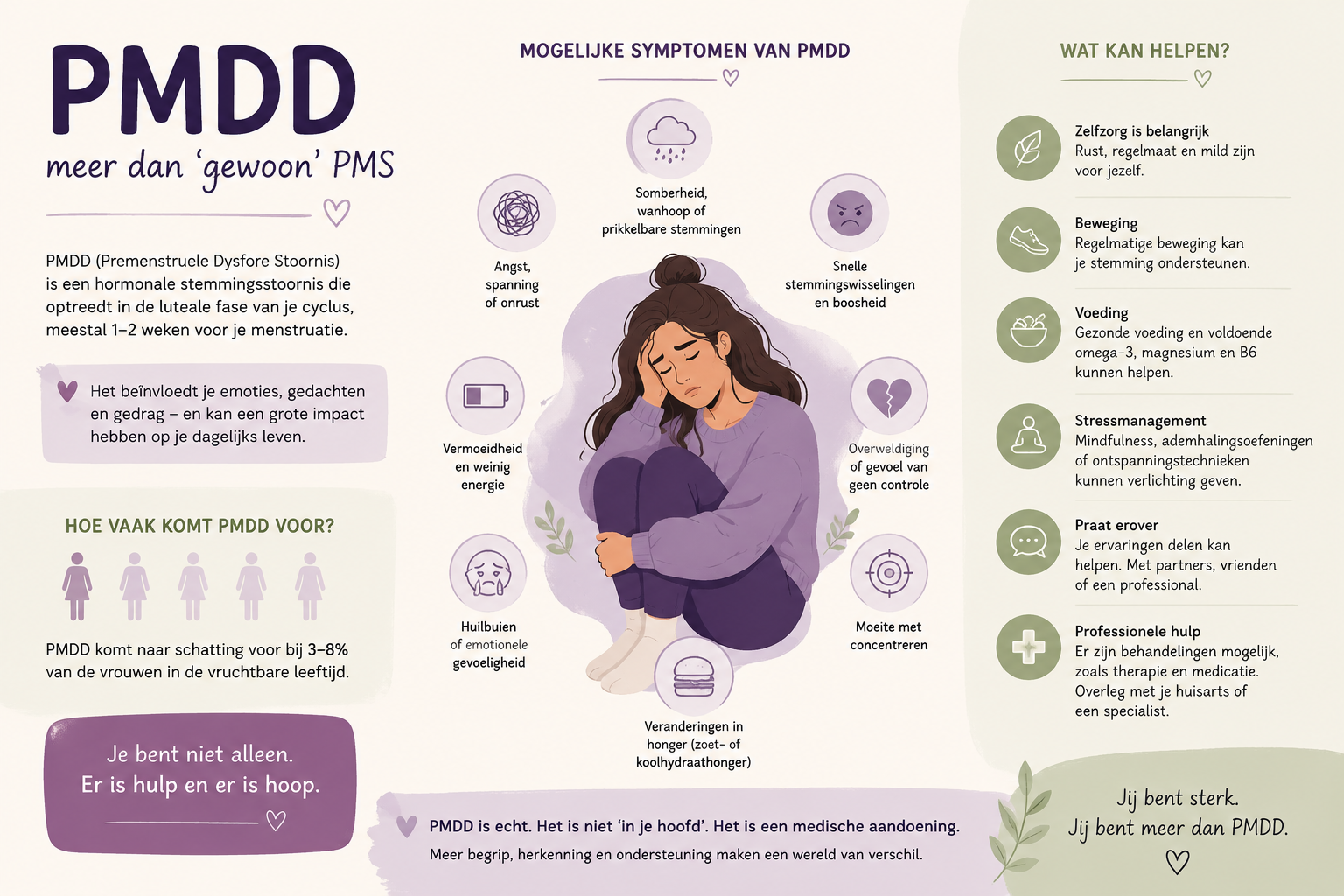
PMDD symptoms are broadly categorized into emotional and physical manifestations. The emotional symptoms are typically the most disruptive and are the primary criteria used for clinical diagnosis.
Emotional and Behavioral Symptoms
- Affective Lability: Sudden, intense shifts in mood, often including crying spells.
- Irritability or Anger: Increased interpersonal conflict or feelings of being “on edge.”
- Depressed Mood: Feelings of hopelessness, worthlessness, or excessive sadness.
- Anxiety: Feelings of being tense, on edge, or overwhelmed.
- Cognitive Changes: Difficulty concentrating or feeling “brain fog.”
Physical Symptoms
- Somatic Tension: Breast tenderness or swelling.
- Digestive Issues: Bloating, abdominal pain, or changes in appetite.
- Sleep Disturbances: Insomnia or excessive tiredness (hypersomnia).
- Physical Fatigue: A general sense of exhaustion or lethargy.
What are the current medical treatment options?
Treatment for PMDD is highly individualized and typically focuses on stabilizing mood fluctuations and managing physical discomfort. Because the condition is linked to the body’s sensitivity to hormonal changes, medical interventions often target the neuroendocrine system.
Selective Serotonin Reuptake Inhibitors (SSRIs) are frequently prescribed to manage the emotional symptoms. Unlike their use in treating chronic depression, some patients find relief using SSRIs only during the luteal phase of their cycle. Hormonal contraceptives may also be used to suppress ovulation and stabilize hormone levels, though their effectiveness varies by individual.
Lifestyle modifications are often recommended as complementary approaches. These include regular physical activity, stress management techniques, and dietary adjustments aimed at stabilizing blood sugar and reducing caffeine and alcohol intake, which can exacerbate mood swings.
Frequently Asked Questions about PMDD
Is PMDD a mental illness?
While PMDD involves significant psychiatric symptoms, it is categorized as a medical condition related to the body’s response to hormonal fluctuations during the menstrual cycle.
Can PMDD be cured?
There is currently no permanent “cure,” but the symptoms can be effectively managed through medication, hormonal regulation, and lifestyle changes.
How long does it take to see results from treatment?
Response times vary. While some patients notice mood stabilization within weeks of starting SSRIs, others may require adjustments to their medication or dosage to find relief.
Patients seeking a diagnosis should consider maintaining a detailed symptom diary for at least two full menstrual cycles to present to their healthcare provider. For further clinical guidance, consulting a gynecologist or a reproductive psychiatrist is recommended.
We encourage you to share this information with those who may be struggling and to join the conversation in the comments below regarding your experiences with reproductive health awareness.
Keep reading