
Syphilis rates among pregnant women in the United States have reached their highest levels since the early 1990s, according to verified data from the National Center for Health Statistics (NCHS). The increase reflects a growing public health concern, as untreated syphilis during pregnancy can lead to severe outcomes for both mother and child, including miscarriage, stillbirth, and congenital infection. Despite being easily detectable and treatable with penicillin, many cases proceed undiagnosed due to gaps in prenatal screening and care access.
The rise in maternal syphilis is closely tied to a concurrent increase in congenital syphilis, where the infection is passed from mother to baby during pregnancy or delivery. Public health officials emphasize that nearly all cases of congenital syphilis are preventable with timely testing and appropriate treatment. Yet, systemic barriers — including lack of insurance, transportation challenges, and clinic closures in rural areas — continue to limit access to prenatal care for millions of women, particularly those from low-income backgrounds and communities of color.
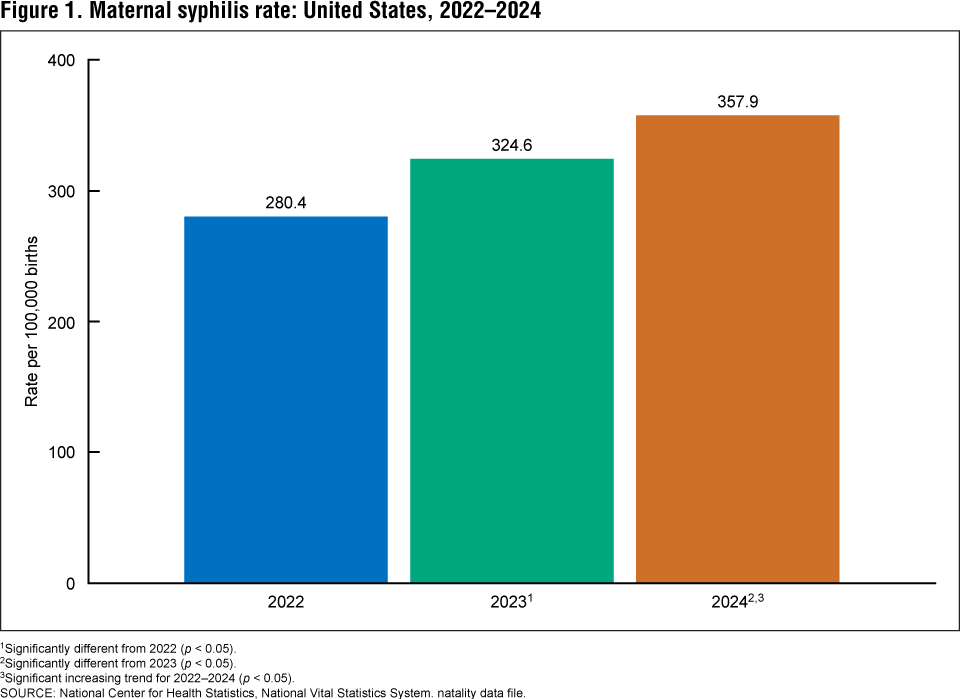
Between 2016 and 2022, the rate of syphilis among pregnant women increased by 222%, followed by an additional 28% rise from 2022 to 2024, according to NCHS data analyzed by the Centers for Disease Control and Prevention (CDC). In 2024, there were 887 cases of maternal syphilis per 100,000 live births among Black women, 411 per 100,000 among Hispanic women, and 188.2 per 100,000 among white women. The highest rates were observed among Native American and Alaska Native women, with 2,145 cases per 100,000 live births.
These disparities underscore long-standing inequities in maternal healthcare access. The CDC reports that 40% of mothers whose babies were born with congenital syphilis in 2022 did not receive adequate prenatal care. In many of these cases, women were either not screened for syphilis despite attending prenatal visits or tested positive but did not receive timely treatment. The agency estimates that 9 in 10 cases of congenital syphilis could have been prevented with proper screening and intervention during pregnancy.
Syphilis, caused by the bacterium Treponema pallidum, often presents no noticeable symptoms in its early stages, making routine screening essential. A simple blood test can detect the infection, and treatment with benzathine penicillin G is highly effective and safe during pregnancy when administered correctly. The American College of Obstetricians and Gynecologists (ACOG) updated its guidelines in 2023 to recommend syphilis screening at three key points: the first prenatal visit, during the third trimester (between 28 and 32 weeks), and at the time of delivery.
This expanded screening approach aims to catch infections that may be acquired later in pregnancy or missed during initial testing. Despite these recommendations, implementation remains inconsistent across states and healthcare systems. While most states mandate syphilis screening at the first prenatal visit, fewer require repeat testing in the third trimester or at delivery, leaving opportunities for prevention unmet.
Access to prenatal care remains a critical factor in preventing congenital syphilis. A 2023 study published in Obstetrics & Gynecology found that approximately 35% of women of reproductive age (15–44) in the United States live in counties without a practicing obstetrician or certified nurse midwife. These maternity care deserts are disproportionately located in rural areas and the South, where hospital closures and provider shortages have reduced access to essential services.
Financial barriers also play a significant role. Women without health insurance or those with high-deductible plans may delay or skip prenatal visits due to cost concerns. Others face logistical challenges, such as taking time off work, arranging childcare, or traveling long distances to reach the nearest clinic. These obstacles are especially pronounced for Black, Hispanic, and Indigenous women, who experience higher rates of poverty and systemic discrimination in healthcare settings.
Public health departments and community organizations are working to close these gaps through mobile clinics, telehealth expansions, and outreach programs that bring testing and treatment directly to underserved populations. The CDC’s “Secure Tested” initiative helps individuals locate free or low-cost STI screening sites, while organizations like March of Dimes and Planned Parenthood offer guidance on accessing prenatal care and support services.
Efforts to raise awareness about the risks of untreated syphilis and the importance of prenatal screening are ongoing. Health officials stress that early detection not only protects the mother’s health but also prevents irreversible harm to infants. Congenital syphilis can cause bone deformities, severe anemia, enlarged liver and spleen, jaundice, and neurological problems such as developmental delays or seizures. In severe cases, it can result in infant death shortly after birth.
As of early 2025, the CDC continues to monitor syphilis trends through its National Notifiable Diseases Surveillance System (NNDSS) and publishes updated surveillance data regularly. The most recent provisional data, released in March 2025, indicates that while the rate of increase has slowed compared to previous years, maternal and congenital syphilis levels remain significantly above historical baselines. Officials urge healthcare providers to adhere to screening guidelines and call on policymakers to invest in expanding maternal healthcare infrastructure, particularly in underserved regions.
For individuals seeking information or testing resources, the CDC recommends visiting gettested.cdc.gov to uncover nearby testing locations. Additional support is available through March of Dimes for maternal health resources and Planned Parenthood for prenatal care services.
Addressing the rise in syphilis among pregnant women requires a multifaceted approach that combines clinical vigilance, equitable access to care, and targeted public health interventions. With proven tools for prevention and treatment available, the continued rise in cases highlights not a lack of medical solution, but a failure to deliver existing care to those who demand it most.
Readers are encouraged to share this information to help raise awareness about the importance of prenatal syphilis screening. Comments and personal experiences related to maternal healthcare access are welcome below.