
For years, the medical community has viewed GLP-1 receptor agonists primarily through the lens of metabolic health—celebrating their ability to tame Type 2 diabetes and combat obesity. However, a groundbreaking shift is occurring in how we perceive these medications. Emerging research suggests that the benefits of these drugs may extend far beyond the scale and blood glucose monitors, potentially offering a lifeline to breast cancer patients struggling with metabolic comorbidities.
The intersection of obesity, diabetes, and oncology has long been a area of concern for clinicians. It is well-established that excess adipose tissue and insulin resistance can create a biological environment conducive to tumor growth. Now, new data indicates that GLP-1 receptor agonists breast cancer survival rates may be significantly improved in patients who also manage obesity or diabetes, suggesting these medications could play a pivotal role in integrative cancer care.
As a physician and journalist, I have followed the rise of “weight-loss drugs” with a mix of curiosity, and caution. While the public focus has remained on cosmetic weight loss, the clinical reality is far more profound. We are seeing the potential for a class of drugs to not only manage a patient’s weight but to fundamentally alter the trajectory of a life-threatening malignancy. This development represents a critical step toward personalized medicine, where metabolic health is treated as a cornerstone of oncological recovery.
The Metabolic Engine of Cancer Growth
To understand why GLP-1 medications are showing promise in oncology, we must first understand the relationship between metabolism and malignancy. Obesity and Type 2 diabetes are not merely comorbidities. they are active contributors to cancer progression. In patients with obesity, the body often produces higher levels of insulin to compensate for insulin resistance—a state known as hyperinsulinemia.
High levels of circulating insulin can act as a growth signal for certain cancer cells, potentially accelerating tumor proliferation and increasing the risk of recurrence. Adipose tissue is not an inert storage depot; it is an active endocrine organ that secretes pro-inflammatory cytokines. This chronic low-grade inflammation can damage DNA and promote an environment where cancer cells can thrive and evade the immune system.
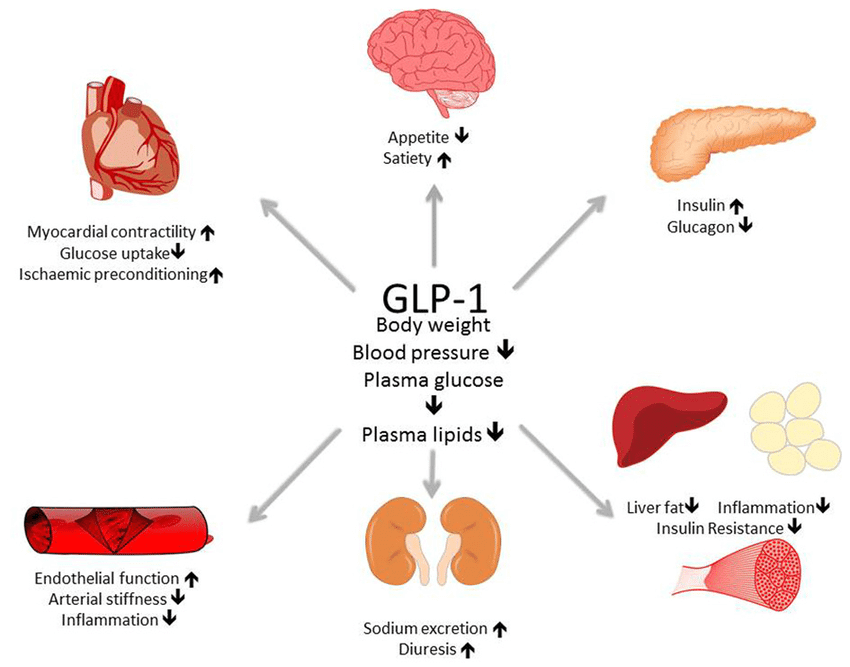
GLP-1 (glucagon-like peptide-1) agonists work by mimicking a natural hormone that stimulates insulin secretion in a glucose-dependent manner, slows gastric emptying, and suppresses appetite. By stabilizing blood sugar and reducing the overall insulin load on the body, these medications may effectively “starve” the growth signals that cancer cells rely on, while simultaneously reducing the systemic inflammation associated with obesity.
New Evidence: GLP-1 RAs and Improved Prognosis
The most compelling evidence for this protective effect comes from recent research published in JAMA Network Open. The study examined the impact of GLP-1 receptor agonists (GLP-1 RAs) on the survival and recurrence rates of breast cancer patients, specifically focusing on those with obesity or diabetes.
The findings suggest that patients utilizing GLP-1 RAs experienced improved survival outcomes compared to those who were not using the medication. Crucially, the research indicates that these benefits are not solely a byproduct of weight loss. While reducing body mass is beneficial, the protective effects appear to stem from the medication’s ability to improve glycemic control and modulate metabolic pathways that directly influence tumor behavior.
This distinction is vital. For many breast cancer patients, drastic weight loss during active treatment can be challenging or even contraindicated depending on their nutritional status. The discovery that GLP-1 RAs may provide oncological benefits beyond mere weight reduction opens the door for these drugs to be used as supportive therapy to improve disease-free survival and overall prognosis in high-risk metabolic groups.
Beyond the Scale: The Biological Mechanism
The potential for GLP-1 receptor agonists to improve breast cancer outcomes likely involves several overlapping biological pathways. Beyond the reduction of hyperinsulinemia, these drugs may influence the “microenvironment” of the tumor. The tumor microenvironment consists of the blood vessels, immune cells, and signaling molecules that surround a cancer cell; if this environment is pro-inflammatory, the cancer is more likely to spread.

Recent insights into medical innovation suggest that GLP-1 RAs may reduce the expression of certain growth factors and inhibit the pathways that lead to angiogenesis—the process by which tumors grow their own blood supply to feed their growth. By restricting this supply and lowering systemic inflammation, the medication may make the cancer more susceptible to standard treatments like chemotherapy and endocrine therapy.
for patients with Type 2 diabetes, the ability to maintain tight glycemic control is essential. Poorly managed blood sugar is often linked to higher toxicity from chemotherapy and a higher rate of post-surgical complications. By providing a more stable metabolic foundation, GLP-1 agonists may allow patients to tolerate aggressive cancer treatments more effectively, thereby improving their overall survival chances.
Integrating GLP-1s into Clinical Cancer Care
Despite these promising results, the integration of GLP-1 receptor agonists into standard oncology protocols must be handled with precision. These medications are not a replacement for primary cancer treatments—such as surgery, radiation, or chemotherapy—but rather a complementary strategy to optimize the patient’s biological terrain.
According to the Cleveland Clinic, GLP-1 agonists are typically administered as subcutaneous injections. For a cancer patient, this means adding another step to an already complex treatment regimen. Clinicians must carefully monitor for side effects, particularly gastrointestinal issues like nausea and vomiting, which can be exacerbated by chemotherapy. Ensuring that a patient maintains adequate nutrition is paramount, as excessive weight loss or muscle wasting (cachexia) can be detrimental to cancer recovery.
The decision to start a GLP-1 RA in a breast cancer patient should be a collaborative effort between an oncologist and an endocrinologist. The goal is to balance the metabolic benefits—reducing insulin resistance and inflammation—with the need to maintain the patient’s strength and nutritional integrity during treatment.
Key Considerations for Patients and Caregivers
- Consultation is Mandatory: Never start a GLP-1 medication for “off-label” cancer benefits without a prescription and direct supervision from an oncology team.
- Nutritional Monitoring: Because these drugs suppress appetite, patients must work with a dietitian to ensure they are consuming enough protein and calories to support healing.
- Comprehensive Care: Metabolic health is one piece of the puzzle; it should be integrated with established breast cancer guidelines and endocrine therapies.
- Individualized Response: Not every patient will respond to GLP-1 RAs in the same way; monitoring of blood glucose and tumor markers remains essential.
The Road Ahead: What This Means for Public Health
The implications of this research extend far beyond a single type of cancer. If GLP-1 receptor agonists are proven to improve survival in breast cancer patients by modulating metabolic signals, it is highly probable that similar benefits exist for other obesity-linked cancers, including colorectal and endometrial cancers.
We are entering an era where “metabolic oncology” could become a recognized sub-specialty. By treating the systemic drivers of cancer—such as insulin resistance and chronic inflammation—rather than just the tumor itself, we can potentially increase the efficacy of existing therapies and improve the quality of life for millions of patients worldwide.
For the global community, this underscores the importance of early intervention in metabolic health. Managing obesity and diabetes is no longer just about preventing a heart attack or a stroke; it is about reducing the risk of cancer and improving the odds of survival should a diagnosis occur.
The next critical milestone will be the results of larger, randomized controlled trials specifically designed to test GLP-1 RAs as adjuvant therapies in oncology. These trials will provide the definitive data needed to update clinical guidelines and potentially make metabolic modulation a standard part of cancer care.
Do you or a loved one manage both a metabolic condition and a cancer diagnosis? We encourage you to share your experiences in the comments below or discuss these emerging findings with your healthcare provider to see if a metabolic approach to care is right for your specific situation.