
A new, locally deployable clinical decision support tool using a case-grounded large language model (LLM) has demonstrated high concordance with hematology tumor board decisions, according to research published in the journal Nature Medicine.
As a physician and health journalist, I often observe that the primary challenge in medical AI is not just raw accuracy, but the ability of a model to ingest specific patient histories and provide outputs that clinicians can actually trust. This development represents a shift toward “case-grounded” AI, which prioritizes the integration of individual patient data over generalized medical knowledge. By operating locally, the system addresses significant concerns regarding data privacy and the security of sensitive genomic and clinical information, which are often barriers to the adoption of cloud-based AI solutions in hospital settings.
The Evolution of AI in Hematology
Hematological malignancies—such as leukemia, lymphoma, and myeloma—often require highly nuanced treatment plans that must account for specific genetic mutations, patient comorbidities, and varying responses to prior therapies. Historically, these decisions have been the exclusive domain of multi-disciplinary tumor boards. These boards, composed of hematopathologists, oncologists, and geneticists, represent the “gold standard” for care but are inherently limited by the time and personnel required to review each case.
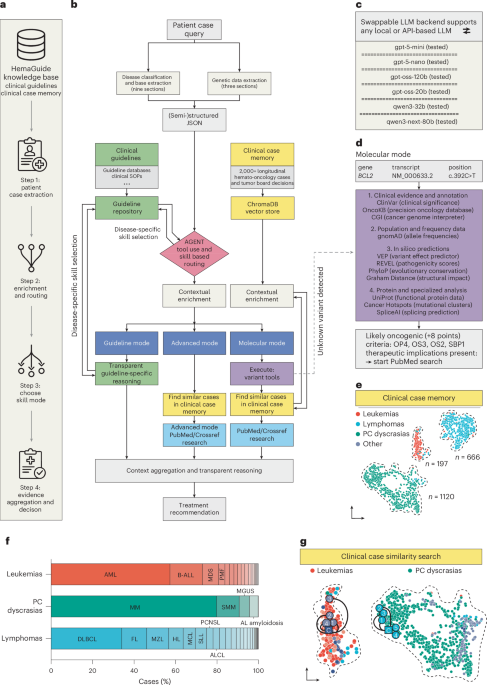
The research published in June 2026 demonstrates that an LLM agent can emulate this decision-making process by grounding its analysis in the specific clinical narrative provided. Unlike standard LLMs that might rely on broad training data, a case-grounded agent acts as a specialized assistant that synthesizes lab results, imaging reports, and patient history into a structured recommendation. This approach aims to reduce the cognitive burden on clinicians while ensuring that treatment plans remain aligned with established institutional guidelines and the most recent clinical trial data.
Performance and Validation Metrics
The system’s performance was rigorously tested across three distinct phases. In the retrospective evaluation, the model analyzed thousands of historical cases, comparing its suggested treatment pathways against the finalized decisions made by human tumor boards. The results showed a high degree of concordance, indicating that the model successfully identified the primary therapeutic strategies favored by human experts in the majority of instances.
External validation further confirmed these findings by testing the model on data from different healthcare institutions, ensuring that the AI was not merely "overfitting" to the specific workflows or terminology of its home facility. Perhaps most significantly, the prospective evaluation—where the model was used as a real-time assistant during live board meetings—demonstrated that clinicians found the AI's suggestions actionable and relevant. The ability to deploy the model locally is a crucial technical detail; it allows hospitals to maintain data sovereignty, a key requirement for compliance with healthcare data protection mandates like the EU’s General Data Protection Regulation (GDPR) and the U.S. Health Insurance Portability and Accountability Act (HIPAA), as detailed by the U.S.
Addressing Clinical Implementation Challenges
Despite these promising results, the integration of LLMs into hematology clinics faces ongoing hurdles. A primary concern is “hallucination”—the tendency of generative AI to produce plausible but factually incorrect information. To mitigate this, the researchers emphasized the importance of the “case-grounded” architecture. By constraining the model to the specific documents provided in the patient’s file, the system is less likely to wander into extraneous medical literature that may not apply to the specific case at hand.
Furthermore, the “human-in-the-loop” model remains essential. The AI is positioned not as a replacement for the hematologist, but as a triage and synthesis tool. It identifies key clinical indicators that might otherwise be overlooked in a lengthy medical chart. For instance, in a complex case of relapsed acute myeloid leukemia, the AI can rapidly cross-reference a patient’s specific cytogenetic profile against emerging clinical trials, presenting a shortlist of options for the human board to review. This keeps the final decision-making power firmly in the hands of the medical team, consistent with current World Health Organization guidance on the ethical use of AI in healthcare.
Future Directions and Regulatory Outlook
The success of this locally deployable agent highlights the potential for “small-scale” AI in specialized medicine. While much of the public conversation around AI focuses on massive, general-purpose models, the clinical reality suggests that specialized, domain-specific tools offer a more reliable path toward patient safety and efficacy. The next steps for the research team involve expanding the model’s capabilities to include a broader range of rare hematological conditions and testing its adaptability to different electronic health record (EHR) systems.
As these tools move toward potential commercialization or wider clinical adoption, they will likely undergo scrutiny from regulatory bodies such as the U.S. Food and Drug Administration (FDA) or the European Medicines Agency (EMA). These agencies are currently developing frameworks for the regulation of “Software as a Medical Device” (SaMD), with a focus on ensuring that models remain accurate even as they are updated with new medical data. Updates on the regulatory status and any upcoming clinical trials will be available through the U.S. National Library of Medicine’s clinical trials registry.
The integration of AI into tumor boards is not an overnight transformation, but a measured evolution. As these systems become more common, the focus will shift from “can AI do this?” to “how does AI improve patient outcomes?” The evidence suggests that when grounded in real-world clinical data, these tools can serve as a powerful force multiplier for hematology teams worldwide.
Do you have experience with AI tools in your clinical practice, or are you interested in how these systems might impact patient care? Share your thoughts in the comments section below.