Respiratory Syncytial Virus (RSV) poses a significant risk to infant health, particularly during the winter months when transmission rates typically climb. As a physician, I frequently emphasize that while RSV often presents as a mild cold in older children and adults, it can progress to severe lower respiratory tract infections, such as bronchiolitis and pneumonia, in premature infants, those with chronic lung or heart conditions, and newborns under six months old. Understanding early intervention and modern preventative strategies remains the most effective way to protect our most vulnerable populations.
According to the Centers for Disease Control and Prevention (CDC), nearly all children will have had an RSV infection by their second birthday. Because the virus is highly contagious and spreads through respiratory droplets, public health officials underscore the importance of vigilant hygiene and, where appropriate, the use of monoclonal antibody prophylaxis for high-risk infants. These clinical measures are designed to bridge the gap in immunity during the critical first months of life.
Identifying High-Risk Populations for RSV
Not every child who contracts RSV will require hospitalization, but medical professionals categorize specific groups as being at higher risk for severe outcomes. Premature infants—those born before 37 weeks of gestation—are particularly susceptible because their lungs are still developing and their immune systems are less robust at birth. Clinical data from the World Health Organization (WHO) highlights that infants with congenital heart disease or chronic lung disease, including bronchopulmonary dysplasia, also face an increased risk of complications that necessitate oxygen therapy or mechanical ventilation.

Age is another primary factor. Infants younger than six months possess smaller airways that are easily obstructed by inflammation and mucus production, which are hallmarks of an RSV infection. Parents should monitor for signs of respiratory distress, such as rapid breathing, wheezing, or “nasal flaring,” where the nostrils widen with each breath. If a child exhibits bluish discoloration around the lips or fingernails, or shows signs of significant lethargy, immediate medical evaluation is required.
Preventative Strategies and Clinical Interventions
Prevention starts with foundational hygiene practices that reduce the viral load in a household. Since RSV can survive for several hours on hard surfaces, frequent handwashing with soap and water and the regular disinfection of toys and high-touch areas are essential. The Mayo Clinic advises limiting exposure to crowds and keeping infants away from individuals who are actively showing symptoms of a cold or respiratory illness.

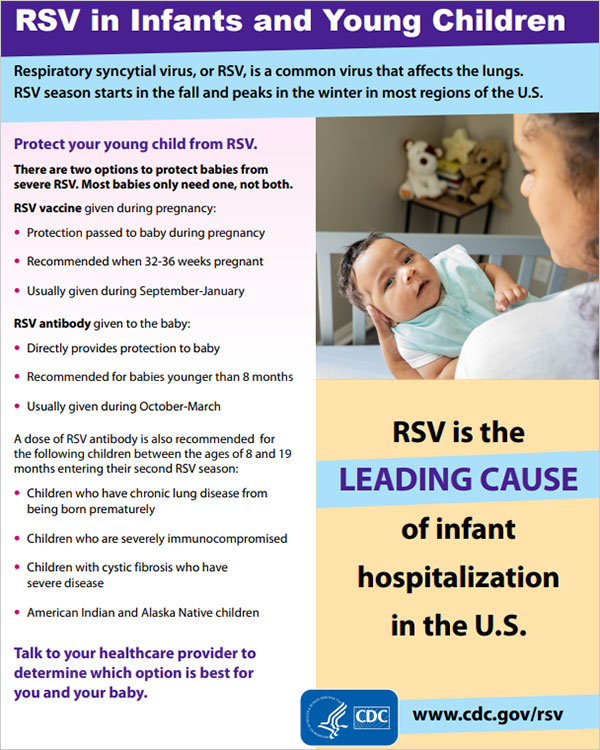
Beyond behavioral changes, the medical community has shifted toward proactive immunological support. For infants at the highest risk, clinicians may recommend monoclonal antibody immunizations. Unlike traditional vaccines that stimulate the body to create its own antibodies, these treatments provide direct, temporary protection by introducing pre-made antibodies into the infant’s system. This approach has become a cornerstone of modern pediatric policy, especially in regions experiencing seasonal surges in viral activity.
Understanding the Role of Maternal Vaccination
An emerging and highly effective strategy for infant protection involves maternal immunization. By administering an RSV vaccine to expectant mothers during the late second or third trimester, the mother develops protective antibodies that are transferred across the placenta to the fetus. This provides the newborn with passive immunity that lasts through the first few months of life, a period when the infant is most vulnerable to severe disease.
The U.S. Food and Drug Administration (FDA) has approved specific vaccines designed for maternal use to prevent lower respiratory tract disease in infants. Discussing this option with an obstetrician or pediatrician allows parents to weigh the benefits based on their child’s expected due date in relation to the peak RSV season. As we continue to refine these clinical pathways, the goal remains consistent: reducing the burden of disease through timely intervention and evidence-based care.
Next Steps for Caregivers
If you suspect your child is struggling to breathe, do not wait for symptoms to worsen. Contact your primary care physician or visit an emergency department immediately. Global health organizations continue to monitor RSV trends, and local health authorities provide seasonal updates regarding the availability of preventative treatments. For the most accurate information tailored to your region, consult your national health ministry’s latest guidelines on seasonal pediatric respiratory infections. We encourage readers to share this information with other parents to help foster a safer environment for our community’s youngest members.

Related reading